
|
March 2025,Volume 47, No.1
|
Update Article
|
Update on antithrombotic therapy in acute coronary syndromeSin-man Li 李善雯, Sunny CS Yue 余朝燊, Charles CH Lo 盧卓恆 HK Pract 2025;47:18-26
SummaryAntiplatelet therapy is the mainstay of treatment in patients who survive acute coronary syndrome (ACS). Balancing the adverse cardiovascular events and bleeding complications could be quite challenging when formulating the antiplatelet therapy. In this article, we will review the latest evidence and recommendations on secondary prevention of ACS, especially in patients with atrial fibrillation. We will also discuss periprocedural management in patients with antiplatelet therapy.
摘要抗血小板治療是急性冠狀動脈綜合症的主要療法。治療急性冠狀動脈綜合症時,要同時平衡心血管疾患和出血併發症的風險,令制定抗血小板治療變得具有挑戰性。本文將探討預防急性冠狀動脈綜合症的最新文獻和建議,特別是針對同時患有心房顫動的人士。另外,亦會討論進行入侵性程序前,抗血小板治療的管理。IntroductionIn Hong Kong, coronary heart disease is the third leading cause of death, which accounts for around 10% of all deaths. Nearly half of these deaths are due to acute coronary syndrome (ACS) and one third of them occur prematurely in people aged < 70 years.1,2 Coronary heart disease is an age-related disease. With the aging population, it is expected that the burden of disease continues to rise. ACS refers to a spectrum of conditions compatible with acute myocardial ischaemia and/or infarction caused by an abrupt reduction in coronary blood flow. It is differentiated into ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation ACS (NSTE-ACS). NSTE-ACS can be further classified into non-ST-segment elevation myocardial infarction (NSTEMI) and unstable angina based on the presence of cardiomyocyte necrosis. Patient is considered to have NSTEMI if necrosis is present as indicated by cardiac biomarker. Otherwise, it is unstable angina.3 Antiplatelet therapy is the cornerstone of secondary prevention of ACS. Family medicine plays an essential role in managing patients with coronary heart disease. Many patients continued the long-term follow-up with their family physicians after ACS. In this review, we are going to discuss the latest recommendations on antithrombotic therapy that are relevant to the primary care practice, in particular the use of antiplatelet for patients with ACS and special considerations on antiplatelet therapy when undergoing surgical or invasive diagnostic procedures. Treatment Approaches of ACSAfter ACS, all patients should receive life-long aspirin.3-5 Efficacy of aspirin in secondary prevention is confirmed by previous meta-analyses in which the absolute benefits outweigh the absolute risks of any major bleeding.6,7 Low-dose aspirin (75 – 100mg daily) was associated with significantly less minor bleeding (i.e. any bleeding requiring modification of the drug regimen but did not fulfil the criteria of major bleeding) and major gastrointestinal bleeding than high-dose aspirin (300 – 325mg daily).8 Major treatment guidelines support the use of low-dose aspirin (75 – 100mg daily) as the maintenance dose for secondary prevention.3-5 Dual antiplatelet therapy (DAPT) consisting of aspirin and a P2Y12 inhibitor are indicated for patients after ACS, regardless of the type of ACS. Proton pump inhibitor is recommended in patients treated with DAPT who are at a high risk of gastrointestinal bleeding.3,5 Clopidogrel, prasugrel and ticagrelor are the oral P2Y12 inhibitors used in the secondary prevention of ACS. Choice of P2Y12 inhibitors would depend on the type of strategy by which a patient with ACS is treated and the genotype of the patient. Patients who underwent percutaneous coronary intervention (PCI), regardless of the choice of stenting, should receive clopidogrel, prasugrel or ticagrelor as part of a 1 year DAPT treatment regimen. Ticagrelor and prasugrel are preferred over clopidogrel due to their better efficacy. Patients with STEMI who received fibrinolysis without subsequent PCI should receive clopidogrel for at least 14 days and ideally for 12 months. For other patients, they should receive either clopidogrel or ticagrelor with aspirin for 1 year. Shortening of DAPT might be considered in selected patients (those who have either a low ischaemic risk or a high bleeding risk).3-5 Elderly patients represent an increasing proportion of ACS. Treatment strategies in the elderly is basically the same as for the younger patients. In those with comorbidities, choice and dosage of antithrombotic agents should be individualised after careful evaluation of risks and benefits.4 Figure 1 summarises the antithrombotic regimens in patients with ACS. Figure 1. Antithrombotic regimens in patients with acute coronary syndrome but without atrial fibrillation3-5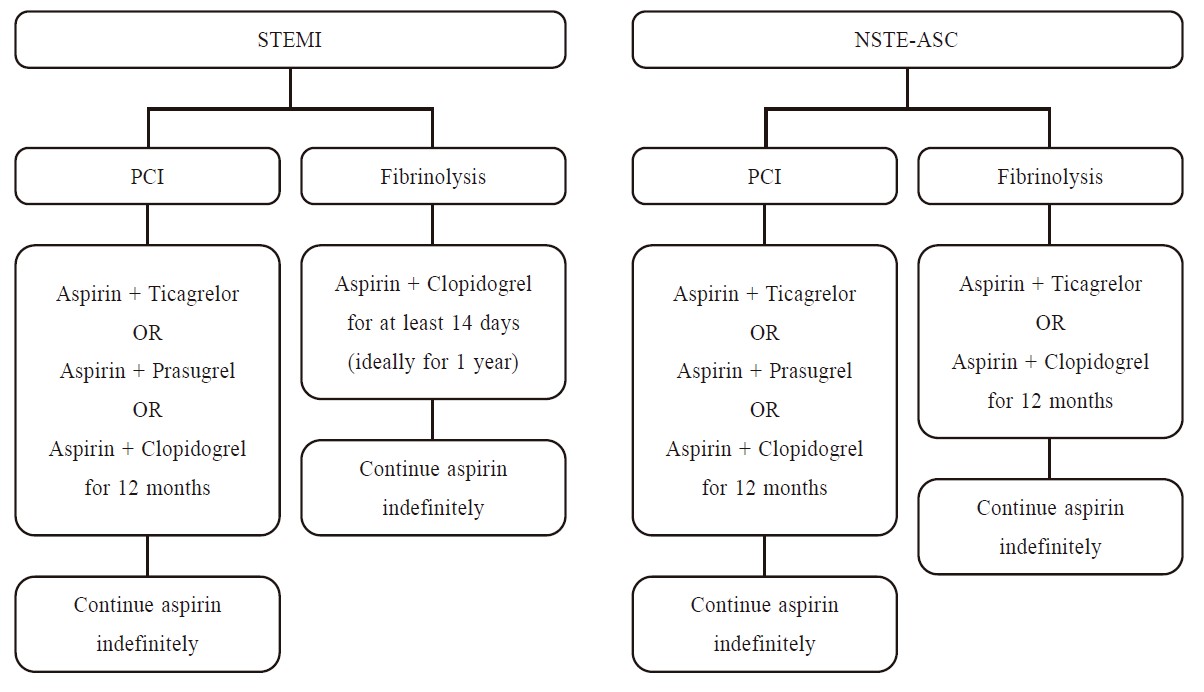
Review of recent guideline updatesEuropean Society of Cardiology 2023 GuidelinesThe European Society of Cardiology updated its clinical practice guidelines for the management of acute coronary syndromes in 2023. General recommendation on DAPT in ACS remains the same. Clopidogrel is preferred in older patients especially for those with a high bleeding risk as defined by the Academic Research Consortium for High Bleeding Risk (ARC-HBR) criteria, such as with chronic kidney disease or anaemia. De-escalation of antiplatelet therapy in the first 30 days after an ACS event should be avoided. In patients with a high bleeding risk, aspirin or P2Y12 inhibitor monotherapy after 1 month of DAPT may be considered. In patients who are event-free and who do not have a high ischaemic risk, single antiplatelet preferably with a P2Y12 inhibitor should be considered after 3 – 6 months of DAPT. P2Y12 inhibitor monotherapy may be considered as an alternative to aspirin monotherapy for long-term treatment in all patients. In patients requiring oral anticoagulation, stopping antiplatelet after 6 months may be considered.3 National Institute for Health and Care Excellence (NICE) 2020 GuidelineNICE guideline on the management of ACS covers both the early and long-term management of ACS. The latest recommendations were released in 2020. Updates of the guideline are mainly on the choice of P2Y12 inhibitor. For patients with ACS who are treated with PCI, prasugrel is recommended as the first line of P2Y12 inhibitor unless aged ≥75. If they have an indication for an oral anticoagulant, clopidogrel is the only choice of P2Y12 inhibitor. For patients with ACS who are not treated with PCI, ticagrelor is preferred over clopidogrel unless they have a high bleeding risk. For patients with an indication for anticoagulation, duration and type of antiplatelet therapy should be taken account into the bleeding risk, thromboembolic risk, cardiovascular risk and patients’ preference. Prasugrel and ticagrelor should not be used in combination with an anticoagulant. The optimal duration of triple therapy is unknown. Anticoagulation and clopidogrel can be used for up to 12 months.4 American College of Cardiology (ACC) / American Heart Association (AHA) 2016 Guideline UpdateThe ACC/AHA Task Force on Clinical Practice Guidelines issued a focused update on the duration of DAPT. In all patients with ACS, DAPT should be given for at least 12 months, regardless of the treatment strategies. Shorter duration DAPT can be considered for those high bleeding risk patients with a low ischaemic risk.5 Review on Oral P2Y12 InhibitorsClopidogrel, prasugrel and ticagrelor are the three oral P2Y12 Inhibitors used as part of DAPT for ACS. Table 1: Oral P2Y12 Inhibitors17,18,22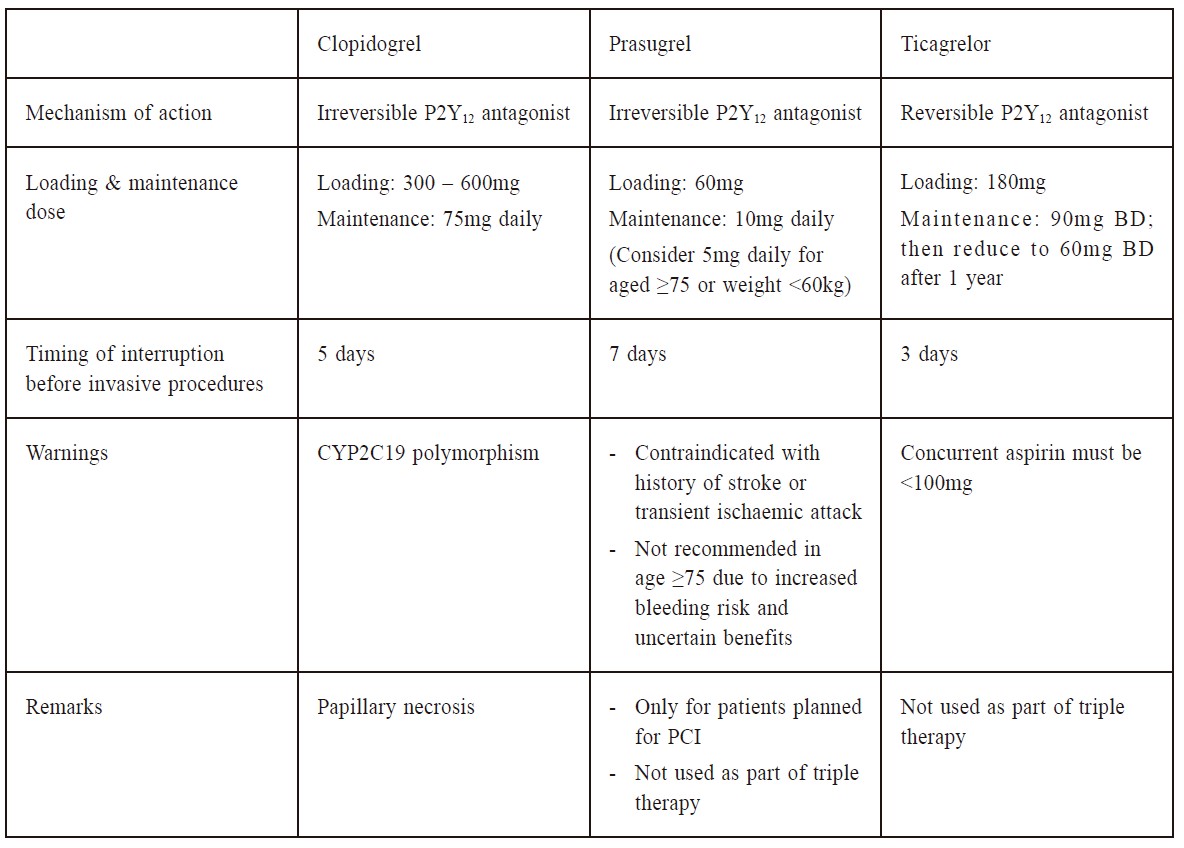
ClopidogreClopidogrel is a prodrug and requires biotransformation to an active metabolite by CYP450 enzymes. The active metabolite irreversibly blocks the P2Y12-adenosine diphosphate (ADP) receptors on platelets, prevents activation of the GPIIb/IIIa receptor complex and reduces platelet aggregation. Landmark studies have established the efficacy and safety of clopidogrel for ACS. In the CURE trial, patients with NSTEMI were randomised to receive either clopidogrel or placebo within 24 hours after the onset of symptoms. They were treated with aspirin concomitantly. Patients receiving combination of clopidogrel and aspirin had a lower primary composite outcome of death from cardiovascular causes, nonfatal MI or stroke (clopidogrel 9.3% vs placebo 11.4%, P< 0.001) but a significant increase risk of major bleeding (clopidogrel 3.7% vs placebo 2.7%, P= 0.001).9 The CLARITY-TIMI 28 trial investigated the use of clopidogrel in patients with STEMI treated with an early medical management strategy. Patients presented within 12 hours of STEMI and planned for fibrinolysis were enrolled and randomised to receive aspirin alone or aspirin plus clopidogrel. Primary outcome was a composite of death or recurrent MI by start of angiography or an occluded infarct-related artery (Thrombolysis in myocardial infarction (TIMI) flow grade 0/1) on angiography. The use of clopidogrel was associated with a significant reduction in primary composite outcome (clopidogrel 15% vs placebo 21.7%, P< 0.001), primarily driven by the reduction in infarct-artery occlusion (clopidogrel 11.7% vs placebo 18.4%, P< 0.001).Major bleeding rates did not differ. (10) Subsequent COMMIT trial also confirmed the efficacy of clopidogrel in STEMI treated medically.11 Optimal duration of clopidogrel therapy following PCI was evaluated in the CREDO trial. Long-term (12-month) treatment of clopidogrel in addition to aspirin was associated with a significant reduction in adverse ischaemic events (relative risk reduction 26.9%, P=0.02).12 Activation of clopidogrel is necessary for its antiplatelet function, which involves CYP450 enzymes particularly CYP2C19. Antiplatelet response to clopidogrel would vary with CYP2C19 genotype. A meta-analysis found that patients with the loss-of-function CYP2C19 alleles had a higher risk of adverse cardiovascular events when treated with clopidogrel compared with an alternative P2Y12 inhibitor. This difference was not observed among patients without the loss-of-function CYP2C19 alleles.13 These observations were replicated in a recent analysis of real-world data.14 CYP2C19 genotype-guided antiplatelet therapy had been suggested to optimise treatment in patients with loss-of-function CYP2C19 alleles.13-16 Prescribing information of clopidogrel highlights the potential impact of CYP2C19 genotype on the pharmacokinetics and clinical response of clopidogrel. Use of another P2Y12 inhibitor in patients identified as CYP2C19 poor metabolisers is suggested.17 Nevertheless, major treatment guidelines did not mention the role of genotype-guided antiplatelet therapy.3-5 CYP2C19 genotype is not routinely checked in the public hospitals in Hong Kong. PrasugrelPrasugrel is rapidly metabolised via CYP450 enzymes, primarily by CYP3A4, CYP2B6 and to a lesser extent CYP2C9 and CYP2C19, to its active metabolite which irreversibly binds to P2Y12-ADP receptors on platelets. Unlike clopidogrel, genetic variation in CYP450 enzymes does not have a relevant effect on the antiplatelet effects of prasugrel.18 In the TRITON-TIMI 38 trial, prasugrel was compared with clopidogrel in patients with ACS planned with PCI. Concurrent use of aspirin at daily doses of 75 – 162mg was required. The primary composite endpoint of death from cardiovascular causes, nonfatal MI or non-fatal stroke was significantly reduced in patients receiving prasugrel (prasugrel 9.9% vs clopidogrel 12.1%, P< 0.001). Clinical benefit of prasugrel tended to be greater in patients with diabetes than those without. However, there was a significant increase in major (prasugrel 2.4% vs clopidogrel 1.8%, P=0.03) and fatal bleeding (prasugrel 0.4% vs clopidogrel 0.1%, P=0.002) in the prasugrel group. Subgroup analysis showed that patients with a previous history of stroke or transient ischaemic attack, aged ≥75 years or weighing < 60kg had no net benefit from prasugrel.19 Followup analysis found that a higher level of the prasugrel active metabolite was found in patients aged ≥75 years or weighing < 60kg.20 Prasugrel is contraindicated in patients with a history of stroke or transient ischaemic attack. Lowering the maintenance dose in patients aged ≥75 years or weighting < 60kg is suggested by the manufacturer, however, this dosage has not been studied prospectively.18 Younger patients, patients with diabetes and patients with a lower risk of bleeding were considered as preferred candidates for prasugrel.5 Use of prasugrel for long-term secondary prevention of NSTEMI / UA without revascularisation was evaluated in the TRILOGY-ACS trial. During the 2.5 years of follow-up, there was no difference in the primary efficacy endpoint between prasugrel and clopidogrel. Higher rates of minor and moderate bleeding were observed in patients taking prasugrel.21 Based on the bleeding risk, prasugrel is not indicated in medically treated ACS.3-5 TicagrelorTicagrelor and its active metabolite reversibly binds to P2Y12-ADP receptors on platelets. Similar to prasugrel, genetic variation in CYP enzymes does not affect the antiplatelet effect of ticagrelor.22 In PLATO trial, ticagrelor was compared with clopidogrel for prevention of vascular events and death in patients with ACS. Primary composite endpoint was defined as death from vascular causes, myocardial infarction or stroke. At 12 months, the primary endpoint occurred less frequently in patient receiving ticagrelor as compared with clopidogrel (ticagrelor 9.8% vs clopidogrel 11.7%, P< 0.001), regardless of whether the patient was planned for invasive management or medical management.23 Subgroup analysis showed that low maintenance doses of aspirin (≤100mg) was associated with better outcomes from ticagrelor.24 Therefore, the daily dose of aspirin should not be more than 100mg when used with ticagrelor. Rates of major bleeding were similar between both groups. Higher discontinuation rate was observed in the ticagrelor users, usually due to dyspnoea.23 An extended duration of ticagrelor use in ACS was evaluated in the PEGASUS-TIMI 54 study. Two doses of ticagrelor, either 90mg BD or 60mg BD, were compared with placebo alone in patients with a history of MI. All patients were co-administered with aspirin. After 3 years, both doses of ticagrelor significantly reduced the incidence of cardiovascular death, MI or stroke (hazard ratio for 90mg of ticagrelor vs placebo 0.85, P=0.008; hazard ratio for 60mg of ticagrelor vs placebo 0.84, P=0.004), but at an expense of having higher rates of major bleeding (P< 0.001 for each dose vs placebo).25 An extended duration of ticagrelor at a reduced maintenance dose may be considered in selected high ischaemic risk patients.4 Managing Antiplatelet Therapy in Patients with Atrial FibrillationThe prevalence of atrial fibrillation (AF) in patients with ACS varies between 2.3 and 21%, with newly diagnosed AF being greater than 7%.26-27 The use of DAPT with oral anticoagulants increases the risk of bleeding by two- to four-folds when compared with either oral anticoagulant alone or DAPT.28-30 In general, the duration of triple therapy (i.e. oral anticoagulant plus P2Y12 inhibitor plus aspirin) should be minimised.3-5 It should be limited to 1 month in high ischaemic risk patients.3 Novel antithrombotic regimens aiming to avoid bleeding complications in patients on oral anticoagulants had been examined (see Table 2). They include regimens involving the use of direct oral anticoagulants, reduced dosage of oral anticoagulant or dual therapy of oral anticoagulant and clopidogrel. In the WOEST study, the safety of dual therapy of warfarin and clopidogrel was compared with triple therapy (aspirin, clopidogrel and vitamin K antagonist (VKA)) in patients with AF and those who have undergone PCI. At 1 year, dual therapy was associated with significantly fewer bleeding events than triple therapy (hazard ratio 0.36, P< 0.0001).31 In PIONEER AF-PCI study, patients with AF undergoing PCI with stents were randomised to low-dose rivaroxaban (15mg daily) plus P2Y12 inhibitor, very-low-dose rivaroxaban (2.5mg BD) plus DAPT, or warfarin with DAPT. Both rivaroxaban groups had a lower rate of clinically significant bleeding than the warfarin group (P< 0.001 for each rivaroxaban dose vs warfarin).32 Similar results were observed in other trials on direct oral anticoagulants. In the open-label randomised controlled multicentre study REDUAL-PCI, warfarin-based triple therapy was compared with dual therapy of dabigatran and P2Y12 inhibitor in patients with AF and who had undergone PCI with stenting. Bleeding events were more common in the triple therapy group than in the dual therapy group.33 The AUGUSTUS study was an open-label 2 x 2 factorial randomised trial comparing the safety of apixaban with VKA and of aspirin with placebo in patients with AF who were planning to use P2Y12 inhibitor after recent ACS or PCI. At 6 months, bleeding event rate was significantly lower in patients receiving apixaban than in those receiving VKA (hazard ratio 0.69, P< 0.001), while it was significantly higher in patients receiving aspirin than in those receiving placebo (hazard ratio 1.89, P< 0.001). Overall, bleeding event rate was highest in VKA/aspirin group (18.7%) and lowest in apixaban/ placebo group (7.3%). More ischaemic events occurred in the placebo group, but these were not statistically significance.34 In the ENTRUST-AF-PCI study, patients with AF undergoing PCI were randomised to either edoxaban plus P2Y12 inhibitor or triple therapy with VKA (aspirin given for 1 – 12 months). The edoxabanbased regimen was non-inferior to triple therapy for bleeding events. The ischaemic events were not significantly different between both groups.35 In summary, novel antithrombotic regimens have been proven to have a lower risk of bleeding than triple therapy. These regimens can be considered in patients who have a higher risk of bleeding (see Figure 2).3-5 Notably, evidence on the risk of stent thrombosis or systemic thromboembolism with those novel antithrombotic regimens was limited. Table 2. Clinical trials of novel antithrombotic regimens in acute coronary syndrome31-35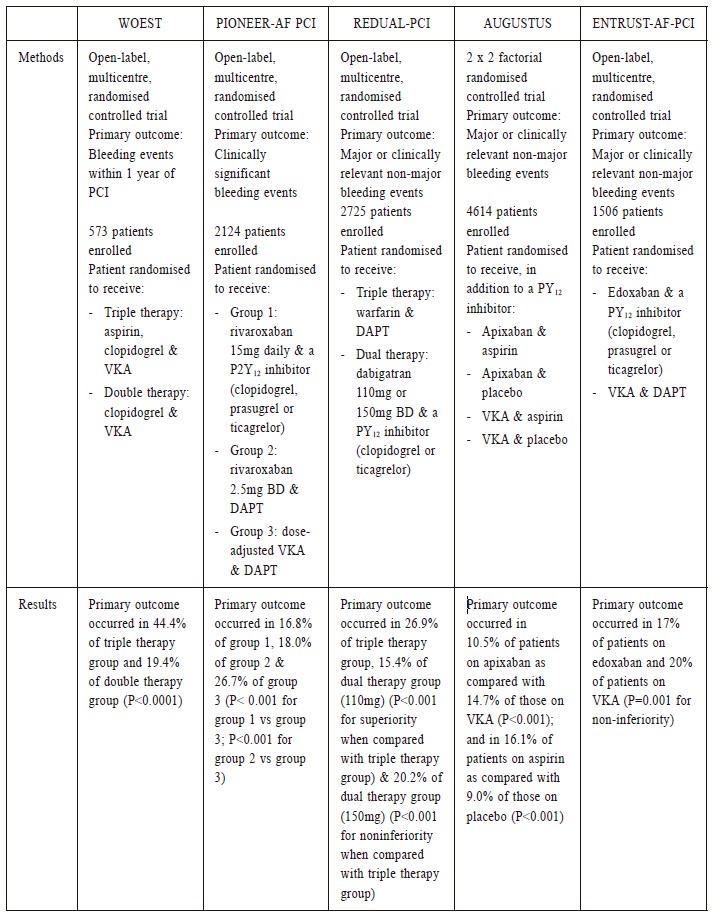
DAPT = Dual antiplatelet therapy; PCI = Percutaneous coronary intervention; VKA = vitamin K antagonist Peri-procedural Management of Antiplatelet TherapyTiming of elective non-cardiac surgical procedures or endoscopic procedures in patients on DAPT involves consideration of the urgency of the elective procedure, the risk of cardiovascular events and the risk of intra- and peri-procedural bleeding if DAPT was to be continued.4,5 Two large observational studies provided information on cardiovascular outcomes in patients with coronary stents who required surgery. A U.S. retrospective cohort study evaluated the incremental risk of non-cardiac surgery on adverse cardiac events after stent placement. Surgical patients within 24 months of stent implantation were matched with nonsurgical patients. Composite cardiac endpoint of MI and/or cardiac revascularisation for the 30-day interval postsurgery was higher in the surgical cohort (P< 0.001). The increased risk on adverse cardiac events was greatest in the first 6 weeks following stent implantation and stabilised after 6 months. The investigators concluded that patients with drug-eluting stent (DES) should delay elective non-cardiac surgery for 6 months after stent placement.36 However, results from later study suggested that surgery after DES placement might be performed earlier without significant risk. In the Danish matched-cohort study, the post-operative rates of adverse cardiovascular outcomes among patients with DES placement were compared with patients without ischaemic heart disease undergoing similar types of surgeries. Patients with DES placement had an increased risk of MI and cardiac death, especially if the surgery was within the first month of DES placement.37 In general, cessation of all antiplatelet therapy should be avoided after PCI with stent placement. Elective non-cardiac surgical procedures may be safely performed within 4-6 weeks after stenting, if surgery cannot be delayed for a longer period.5,38 Consider postponing elective non-cardiac surgery for up to 6 months in patients with recent MI or other high ischaemic risk features.4,5 The ACC/AHA recommends to delay elective non-cardiac surgery for at least 30 days after bare metal stent placement and at least 3 months after DES placement.5 The American Society for Gastrointestinal Endoscopy recommends to delay elective endoscopic procedure up to 12 months after DES placement if clinically acceptable.39 P2Y12 inhibitors should be withheld before surgical procedures or endoscopic procedures in patients on DAPT, while aspirin should be continued. Discontinuation of P2Y12 inhibitors before invasive procedures would depend on their half-lives, at least 3 days for ticagrelor, at least 5 days for clopidogrel and at least 7 days for prasugrel. P2Y12 inhibitors should be resumed as soon as possible when haemostasis is achieved or within 24 hours after the procedure.4,5,38 Figure 2. Antithrombotic regimens in patients with acute coronary syndrome and atrial fibrillation3-5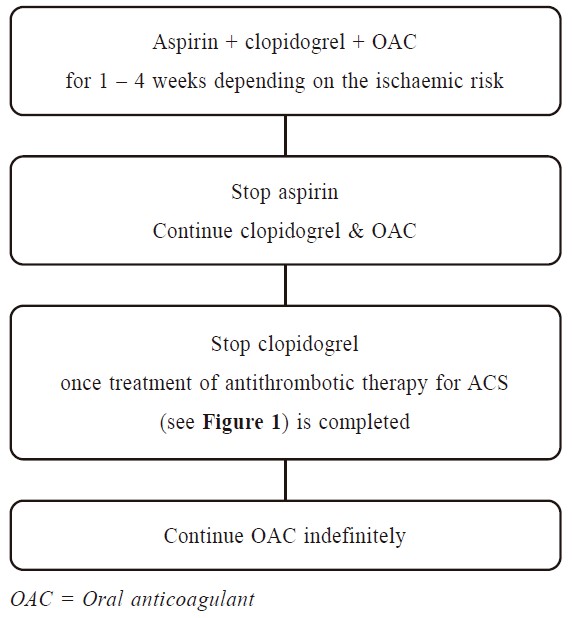
Key messages
ConclusionsDAPT is the mainstay of treatment in all ACS survivors. Clopidogrel, prasugrel and ticagrelor are approved for the secondary prevention of ACS. Choice and duration of DAPT would depend on the type of treatment strategy and the presence of AF. The patients’ genotype is a new aspect to be considered when formulating DAPT. During transition of care, family physicians have a unique role by working collaboratively with cardiologists to ensure that patients are receiving antiplatelet drugs for the appropriate duration. Patients with a high risk of gastrointestinal bleeding should be given a proton pump inhibitor in combination with DAPT. Family physicians may refer patients to elective non-cardiac surgical procedures or diagnostic endoscopic procedures, in general, - these should be avoided for at least 4 weeks after ACS in patients on DAPT. Aspirin should be continued while P2Y12 inhibitors should be withheld timely before the procedures. References
Sin-man Li,
BPharm(Hons) (CUHK), MSc (University of London, UK), BCPS (Board of Pharmacy
Specialties, US), BCACP (Board of Pharmacy Specialties, US)
Sunny CS Yue,
MB ChB(CUHK), MRCP(UK), FHKCP, FHKAM(Medicine)
Charles CH Lo,
BPharm(Hons) (University of Bath, UK), MClinPharm (CUHK), MSc (University of
Birmingham, UK)
Correspondence to: Ms. Sin-man Li, Department of Pharmacy, G/F, S Block,
|
|