
|
March 2025,Volume 47, No.1
|
Case Report
|
An uncommon cause for a common complaint: 2 case of Pancoast tumour presented as shoulder painJing Hou 侯婧, Derek GC Ying 邢格政, Catherine XR Chen 陳曉瑞 HK Pract 2025;47:3-7 SummaryShoulder pain is one of the most common causes for patients seeking for medical care in primary care settings. We herewith report two cases of shoulder pain caused by Pancoast tumour, a rare type of lung cancer located in the apex of the lung. Early diagnosis can be challenging due to the lack of respiratory symptoms and the clinical signs may mimic musculoskeletal pain. The vastly contrasting prognosis of these two cases highlighted the importance of distinguishing extrinsic causes from intrinsic causes of shoulder pain. A chest X-ray, on top of shoulder imaging, is a simple investigation and is potentially life-saving, especially for those with risk factors of lung cancers.
摘要肩膊痛是普通科門診最常見的主訴之一,我們報告兩例因Pancoast 腫瘤引發肩膊痛的患者。Pancoast 腫瘤是位於肺尖的一種罕見肺癌。因為患者通常缺乏肺部症狀,而且表現同常見的肩膊痛和頸椎病很相似,所以早期診斷比較困難。這兩例患者的不同預後強調了在肩膊痛的患者中甄別出肩關節外病因的重要性。特別是針對有肺癌危險因素的患者,在做肩部檢查的同時加一張簡單的肺片可能會挽救病人的生命。 IntroductionShoulder pain is the third most common musculoskeletal presentation in primary care after back pain and knee pain.1 Although the most common underlying causes are, in their order of prevalence, rotator cuff disorders (85% of cases), glenohumeral disorders ,and acromioclavicular joint (ACJ) pathologies1, the first step in the diagnostic approach should always be to exclude extrinsic causes from the neck, chest (including both cardiovascular and thoracic diseases) and abdomen. We present two cases of shoulder pain caused by a rare aetiology of Pancoast tumour with contrasting prognosis. Case 1Mr. LKM, 62-year-old Chinese gentleman and chronic smoker of 40-pack years, presented to a General Outpatient Clinic (GOPC) on 5/5/2021 with progressive right shoulder pain for 4 months. He worked as a security guard and enjoyed good past health. The pain started insidiously over the whole right shoulder, gradually progressed to right arm, right anterior upper chest and upper back, with right upper limb numbness and weakness. There was no prior history of shoulder injury. He visited his general practitioner and bone setter several times and was treated as frozen shoulder after unremarkable shoulder X-ray findings. Despite several courses of analgesics and serial sessions of physiotherapy, the right shoulder pain persisted. The unremitting resting pain and nocturnal pain had significantly affected his work and sleep. Furthermore, he developed hoarseness of voice, right neck swelling, mild dysphagia and weight loss of over 20-pound in 3 months. Otherwise, there was no fever, cough, chest pain or dyspnoea all along. On physical examination, his vital signs were stable. Neck exam revealed diffuse fullness over the right supraclavicular fossa and slightly dilated distended neck vein, without any palpable mass or lymph nodes. The right shoulder was normal in inspection without muscle wasting and there was no tenderness on palpation. The active range of motion of the right shoulder was full. The power of right deltoid muscle was reduced (4 out of 5). There was no facial swelling or Horner’s sign (ptosis, miosis or anhydrosis), nor finger clubbing. The rest of his physical examination was unremarkable. In view of these alarming symptoms and signs, he was urgently referred to the Accident and Emergency Department (AED) for further management. Chest X-ray (CXR) showed a right apical mass with right upper lobe collapse and right 1st rib destruction (Figure 1). Ultrasound of the neck revealed that upper part of right brachiocephalic vein, proximal right internal jugular and right subclavian veins were distended and thrombosed. PET-CT suggested that there was a mass 8.0 x 5.9 x 7.2 cm in size over right upper lobe, with adjacent pleura, upper mediastinum and right chest wall invasion (Figure 2). Metastasis were noted in bilateral adrenal, left chest wall intramuscular, right humeral focal bone and right hilar lymph node. Figure 1. CXR of Mr. LKM: the right paratracheal stripe were thickened and dense, with an apical mass measuring up to 3.5 cm (arrow).
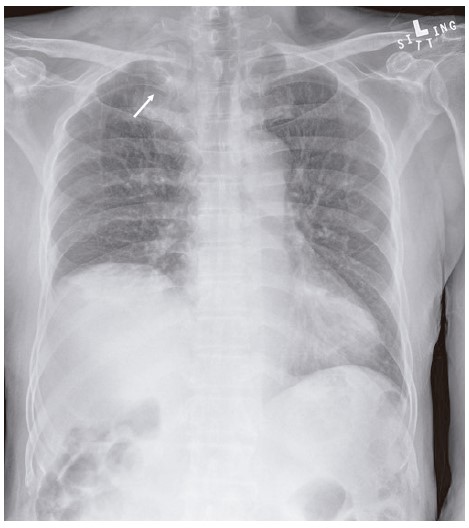
Figure 2. CT Thorax of Mr. LKM: A large irregular lobulated tumor noted at right lung apex (arrow) with central necrosis and destruction of right first rib.
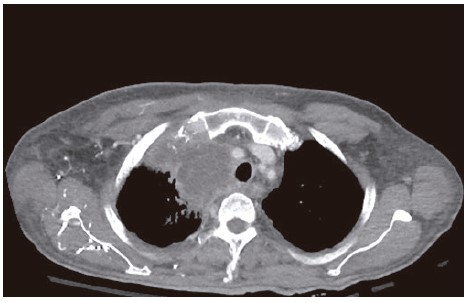
Figure 3. PET-CT of Mr. LKM: A large, moderately hypermetabolic mass (8.0 x 5.9 x 7.2 cm) in the right upper lobe (arrow), with central necrosis. Invasions of the adjacent pleura, upper mediastinum, and right anterior chest wall including the first rib were noted.
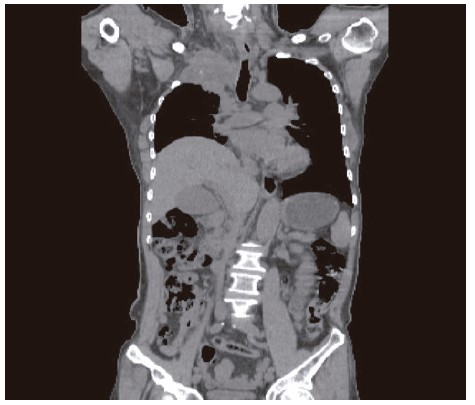
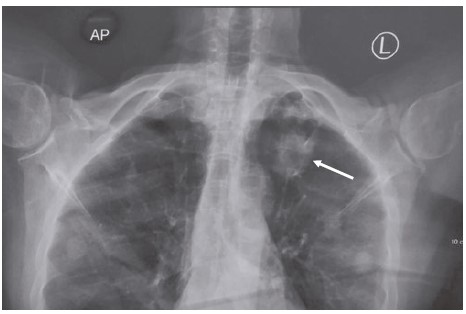
Figure 4. CXR of Madam TLK: A round opacity of 3cm in size over left apex.
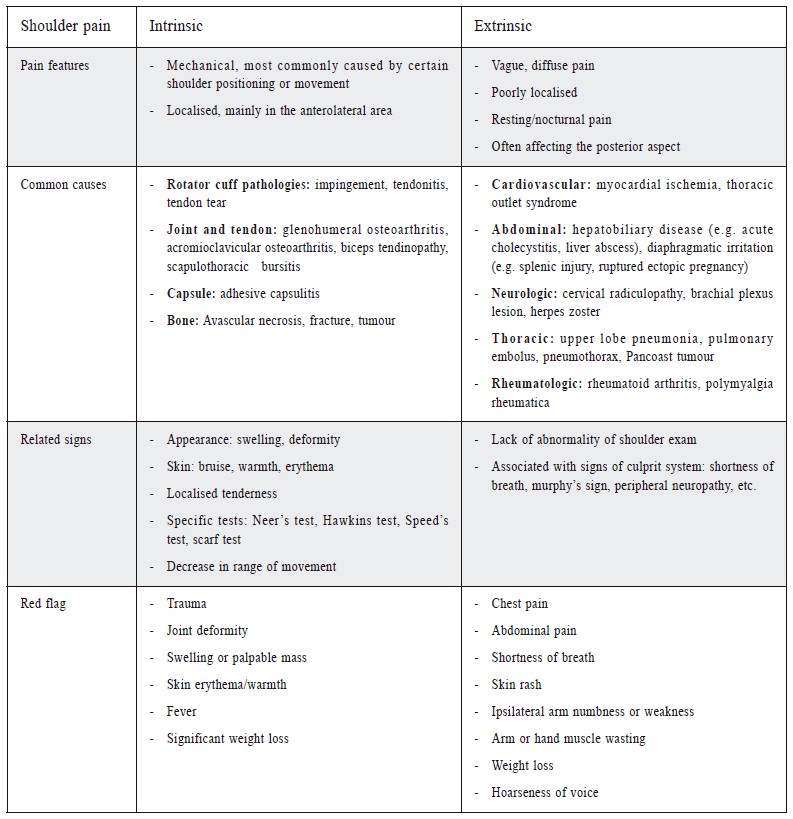
In view of the late stage of malignancy, Mr. LKM was considered not a good candidate for surgery. A subsequent bronchoscopy failed to obtain any positive tumour tissue. While waiting for the fine needle aspiration (FNA) biopsy, the patient developed delirium and facial swelling due to left frontal lobe infarct and superior vena cava (SVC) obstruction. Urgent SVC stent insertion was uneventful, and final FNA confirmed lung adenocarcinoma with negative epidermal growth factor receptor (EGFR)/anaplastic lymphoma kinase (ALK)/ proto-oncogene tyrosine-protein kinase (ROS-1) and 70% programmed death-ligand 1 (PDL-1) expression. Patient’s condition gradually deteriorated, and he succumbed 4 months after his consultation in GOPC. Case 2Madam TLK, a 70-year-old Chinese lady, presented to GOPC on 11/5/2021 with a 10-day-history of left shoulder pain. She was an ex-smoker and quitted smoking 15 years ago. She enjoyed good past health. The left shoulder pain was vague but persistent, radiating to her left upper back, with nocturnal pain and left arm numbness. She denied any history of injury, cough, fever or skin rash. Physical examination was unremarkable. Considering her age, history of smoking, symptoms suggestive of extrinsic causes of shoulder pain, a CXR was ordered along with left shoulder radiograph. Left shoulder radiograph showed calcific tendonitis; and CXR revealed a 3 cm opacity in the left upper zone (Figure 4). Further CT thorax and PET-CT scan arranged in private confirmed left apical lung cancer without evidence of distant metastasis. Left upper lobectomy was performed in a private hospital the following week. The final diagnosis was stage IIb left lung adenocarcinoma with positive expression of EGFR and negative ALK/ROS-1/Kirsten rat sarcoma viral oncogene (KRAS) and PDL-1. She received 3-month adjuvant osimertinib therapy, and opted for conservative treatment and surveillance afterward. Hitherto, one and half years after the diagnosis of Pancoast tumour, her condition has been stable with no evidence of recurrence. DiscussionPancoast tumour, also known as a superior sulcus tumour, is an uncommon lung cancer located at the pulmonary apex, representing 3-5% of lung cancers.2 It originates from the apical pleuro-pulmonary groove, and invade the surrounding structures, including the 1st to 3rd ribs, vertebral bodies, brachial plexus and subclavian vessels. Consequently, Pancoast tumour causes a constellation of signs and symptoms characterised by ipsilateral shoulder and arm pain, cervical radiculopathy (C8 to T1 are commonly involved), hoarseness of voice, Horner’s syndrome and superior vena cava syndrome. Pain in upper extremity, shoulder pain in particular, is its most common initial symptom. As such, Pancoast tumour is often misdiagnosed as musculoskeletal pain in the early stages, resulting in a delayed diagnosis and management for three to more than nine months.3-6 When attending patients with shoulder pain, particular attention should be paid to red flags symptoms that are suggestive of an extrinsic cause such as tumour, infection, fracture or neuropathy. For example, shoulder pain due to extrinsic causes is usually vague, diffuse and poorly localised, affecting the posterior aspect more and is associated with resting pain or nocturnal pain. There is usually no prior history of trauma or sprain and the disease onset could be quite insidious. This is in contrast with the mechanical pain which is usually localised and involves the anterolateral aspect of the shoulder more if the pain is due to joint pathology itself. In addition, there is usually a trauma or overuse history for intrinsic shoulder pain, which might have triggered the relatively acute onset of shoulder pain. Concerning the signs, shoulder pain due to intrinsic causes usually has a localised tenderness when elicited and relevant stress test will be positive depending on the part of joint, muscle or tendon involved. For shoulder pain due to extrinsic reasons, however, the shoulder exam is usually normal but there are other positive findings from the culprit system involved. The differentiating features of the intrinsic and extrinsic causes of shoulder pain is summarised in Table 1. For our cases, both cases suffered from vague, poor localised, non-mechanical shoulder pain with arm numbness, resting pain and nocturnal pain. All these features were compatible with an extrinsic entity of shoulder pain. Unfortunately, case 1 presented to us quite late (4 months after symptoms onset) due to various reasons. With such advanced staging, Mr. LKM passed away 4 months after the confirmed diagnosis despite all efforts. Based on the experience from case 1, we quickly recognised the differentiating features hence an additional CXR was timely ordered. Madam TLK’s prognosis improved tremendously because the correct diagnosis was made at a very early stage. These two cases have clearly illustrated the great importance in differentiating the intrinsic shoulder pain from extrinsic shoulder pain as the first step of diagnostic approach of shoulder pain in our daily practice. Table 1: Characteristics of intrinsic and extrinsic causes of shoulder pain
Non-small cell carcinomas are responsible for over 90% of Pancoast tumour. Among them, adenocarcinoma surpassed squamous cell carcinoma as the leading histological type.2 The risk factors of Pancoast tumour are akin to those for lung cancer, which include smoking or second hand smoke exposure, exposure to radon or occupational hazards, and a family history of lung cancer. The reported average age at presentation is around 60 years; and men are more frequently affected than women.7 Clinicians should remain vigilant of this aetiology which commonly masquerades as shoulder musculoskeletal pain; and thorough history taking, focused physical examination, and maintaining a broad spectrum of differential diagnoses are critically important in its detection. Once suspected, CXR can be a simple and convenient method to start with. The effectiveness of CXR in early detection of small tumour in asymptomatic patients is limited; but for symptomatic patients with history as short as 10 days, such as our Case 2, CXR is sensitive in detecting pulmonary opacity over apex. Apico-Lordotic view of CXR, and radiographs of the cervical and upper thoracic spine may also be helpful. For highly suspicious cases, or when there is an asymmetry of greater than 5 mm in the apices on plain CXR warrants further investigations such as CT scan or MRI. Key messages
The prognosis for Pancoast tumour is gloom, as this disease is invasive to adjacent structures by definition, and the diagnosis is usually late in the course as presented in our case 1. Less than 50% of cases are fit for surgical operation at presentation.7 The average 5-year-survival rate was 30%8 and the median survival was 6.4 months9 if the tumour is staged T4 with invasion to brachial plexus, vertebral bodies or vascular structures. As shown in our case report, prognosis of the two cases were vastly contrasting because of the significant difference in tumour stage (stage IV vs stage IIb). Early diagnosis is always crucial for survival. As long as the doctors are familiar with the red flag signs of shoulder pain, investigation should be timely arranged to rule out the underlying severe diseases or malignancy accordingly. We hope this case report will enhance primary care doctors’ awareness on this rare aetiology of shoulder pain so that correct diagnosis can be made at an early stage and patients’ prognosis could be prominently improved. ConclusionPancoast tumour is a rare type of apical lung cancer that causes ipsilateral shoulder pain. Since shoulder pain is one of the most common symptoms encountered in primary care, family physicians should stay on the lookout for “red flag” signs of shoulder pain, especially for men in their 60s with a smoking history. For suspected cases, an additional CXR is a practical and convenient investigation in primary care to detect the apical abnormality. Vigilance from primary care physicians and early simple investigation can lead to timely diagnosis and improved prognosis. References
Jing Hou,
PhD (Public Health, CUHK), FHKAM (Family Medicine), FHKCFP, FRACGP
Derek GC Ying,
LMCHK, FHKAM (Family Medicine), FHKCFP, FRACGP
Catherine XR Chen,
PhD (Med, HKU), MRCP (UK), FRACGP, FHKAM (Family Medicine)
Correspondence to:
Dr. Jing Hou, Room 622, Nursing Quarter, Queen Elizabeth Hospital,
|
|