
|
June 2025,Volume 47, No.2
|
Case Report
|
Psoriatic arthritis presented with polyarthritis without a history of psoriasis – a diagnostic challenge for primary care doctorsPui-kwan Chan 陳佩君, Derek GC Ying 邢格政, Catherine XR Chen 陳曉瑞 HK Pract 2025;47:44-49 SummaryPsoriatic arthritis (PsA) is an inflammatory arthritis associated with psoriasis. It commonly presents as asymmetrical oligoarthritis or polyarthritis in patients with a known history of psoriasis. However, patients may present with joint symptoms before the onset of any psoriatic skin lesions, rendering PsA a diagnostic challenge for primary care doctors. We report a case of a 34-year-old gentleman who presented with polyarthritis without obvious psoriatic skin lesions. A subtle psoriatic plaque was subsequently identified by rheumatologists and the diagnosis of PsA was ascertained. The patient was started on Disease Modifying Anti-rheumatic Drugs (DMARDs) and tumour necrosis factor (TNF) inhibitor. This case report illustrates the importance of a thorough and systematic approach in the diagnostic process of polyarthritis.
摘要銀屑病關節炎(PsA)是一種與銀屑病相關的炎症性關節炎。 在有已知銀屑病史的患者中,它通常表現為不對稱的寡關節炎或多發性關節炎。然而,患者可能在出現任何銀屑病皮膚病變之前就出現關節症狀,這使得PsA對基層醫療醫生來說成為一個診斷難題。 我們報告了一位34歲的先生,他患有多發性關節炎,沒有明顯的銀屑病皮膚病變。 隨後,風濕病學家發現了一個細微的銀屑病斑塊,並確定了PsA的診斷。 患者開始服用改善病情的抗風濕藥物(DMARDs)和腫瘤壞死因子(TNF)抑制劑。本病例報告說明了在多關節炎診斷過程中採用全面且有系統的方法的重要性。 IntroductionPolyarthralgia is a common presenting complaint in our clinical practice. The list of differential diagnosis can be extensive, ranging from self-limiting causes such as reactive arthritis, to disabling rheumatologically conditions such as rheumatoid arthritis (RA) and PsA. PsA is an inflammatory arthritis associated with psoriasis. It affects women and men at an equal ratio. The prevalence of PsA ranges from 0.1 to 1% worldwide and is lower in Asia (China 0.002%).1 It is a diagnosis that is frequently missed. A recent population based study demonstrated that more than half of PsA patients had a delay in diagnosis of two or more years.2 Several factors contribute to a delay in making the diagnosis of PsA; these include a lower awareness of PsA compared to RA and a lack of a gold standard diagnostic test for PsA.3 Arthritis symptoms onset prior to psoriasis in a portion of PsA patients also pose additional difficulty with this diagnosis. Through this case sharing, we hope to reacquaint readers with the different causes of polyarthritis, with a specific focus on the diagnosis of PsA. The caseMr. LKH is a 34-year-old gentleman. He had been working as a construction site worker for several years. He was a non-smoker and non-drinker, and was regularly followed up in a General Out-patient Clinic (GOPC) of the Hospital Authority (HA) of Hong Kong for management of hyperlipidaemia which did not require pharmacological treatment. He has no other significant past medical history. He was seen on 16/4/2022 during a routine followup for his hyperlipidaemia in GOPC. He complained of right wrist and middle finger proximal interphalangeal joint (PIPJ) pain for 6 months which were associated with swelling and morning stiffness. The arthralgia was present at rest and exacerbated with movement. He further disclosed resting and mechanical pain in his left knee of a similar duration. The knee arthralgia was migratory and had recently spread to his contralateral knee and bilateral hip joints. There was no history of trauma, and no triggering factors were identified to explain his joint symptoms. The patient denied any rash, oral or genital ulcers, Raynaud phenomenon, eye or bowel symptoms. Other systemic symptoms were also absent. There was no known family history of RA or other autoimmune diseases. His migratory polyarthralgia was progressive, and intensified to an extent that he attended the Accident and Emergency Department (AED) of HA Hospital on 13/4/2022. Plain radiographs of his right wrist and right middle finger performed in AED showed no fracture with normal bone alignment and joint spaces. The only abnormality noted in the X-rays was soft tissue swelling at his right 3rd PIPJ. Patient was started on nonsteroidal anti-inflammatory drug (NSAID) in AED and was r ef er r ed to the Medical Specialist Outpatient Department for further management. However, despite the use of NSAID, the polyarthralgia was so disabling that the patient had to quit his job as a construction site worker. On physical examination, his general condition was well and he was afebrile. He was obese with a BMI of 31.4 kg/m2. Examination of his hands revealed active synovitis in multiple joints, including a diffusely swollen tender right wrist, a swollen right 3rd PIPJ with mild flexion deformity, and a mildly swollen left 4th PIPJ with minimal tenderness (Figure 1). Bilateral knees and hips examinations were unremarkable. The finger nails were normal with no obvious pitting, discoloration or Beau’s lines. There was no obvious skin rash over his face, limbs and trunk. Figure 1. Clinical photo of patient showing swollen right middle finger PIPJ with mild flexion deformity, and mildly swollen left ring finger PIPJ

His inflammatory markers were elevated with an Erythrocyte Sedimentation Rate (ESR) level of 66 mm/ hr (normal range < 10 mm/hr) and C-Reactive Protein (CRP) level of 30.3 mg/L (normal range < 5.0 mg /L). His white blood cell level was mildly elevated at 12.2 x 109 /L (normal range 3.7-9.3 x 109/L). Other blood tests including liver function, renal function, calcium and phosphate levels, and urate level were all normal. Autoimmune markers including rheumatoid factor (RF), anti-cyclic citrullinated peptide antibody (ant- CCP Ab) and anti-nuclear antibodies were unremarkable. Human leukocyte antigen B27 (HLA B27) was not detected. In view of his progressive and disabling joint symptoms, the patient was referred to the rheumatology specialist for further evaluation. The patient was subsequently seen by a private rheumatologist in May 2022. Psoriatic plaques were found over the patient’s scalp and post-auricular regions (Figure 2a and 2b). He was therefore diagnosed to have scalp psoriasis with psoriatic arthropathy. All along, the patient was unaware of the presence of these plaques. He was started on Cyclosporine A 100mg two times per day, Prednisolone 10mg daily and Arcoxia 90 mg per day. The patient was referred back to the Hospital Authority Rheumatology team for further management; where Methotrexate and TNF inhibitor were started in view of his progressive disease and persistent joint damage. He was also referred to physiotherapist for symptomatic relief and the dietitian for body weight reduction. Figure 2a and 2b. Clinical photos showing the scaly patches over patient’s post-auricular region and scalp

DiscussionPolyarthralgia is a commonly encountered chief complaint in our clinical practice, but identifying its underlying cause may not be straightforward due to an extensive range of differential diagnosis. In this case report, we share a case of a young man with polyarthritis that posed a diagnostic challenge to primary care physicians. As the patient did not volunteer the history of skin rash, the absence of a systematic diagnostic approach to polyarthralgia has led to a delayed diagnosis of PsA for this patient. This case highlights the need for Family Physicians to formulate a systematic approach in order to make timely diagnosis of important autoimmune diseases presented as polyarthralgia. Joint pain can be inflammatory or non-inflammatory in origin . While non-inflammatory arthritis is predominantly related to degeneration, inflammatory arthritis is characterized by warm and swollen joints, associated with prolonged morning stiffness. Polyarthritis is a term used when at least five joints are affected with inflammatory arthritis. Differential diagnoses of polyarthritis and their clinical features are summarized in Table 1. It calls for an active review of systems during history taking and physical examination to narrow down the scope of possible diagnoses. Psoriasis is a chronic inflammatory skin disease. The classic cutaneous manifestation of psoriasis is erythematous, scaly and well demarcated plaques over the extensor surfaces (elbow and knee). They are also frequently found in hidden areas including the scalp, post-auricular region, umbilicus, intergluteal cleft and skin folds. Lesions begin as erythematous papules with mild scaling that gradually enlarge into rich red plaques. The plaques vary in size and patients may present with only a few lesions in mild disease, while psoriatic plaques may involve the majority of the body surface area in severe cases. Table 1: Differential diagnoses of polyarthritis and their clinical features and laboratory findings
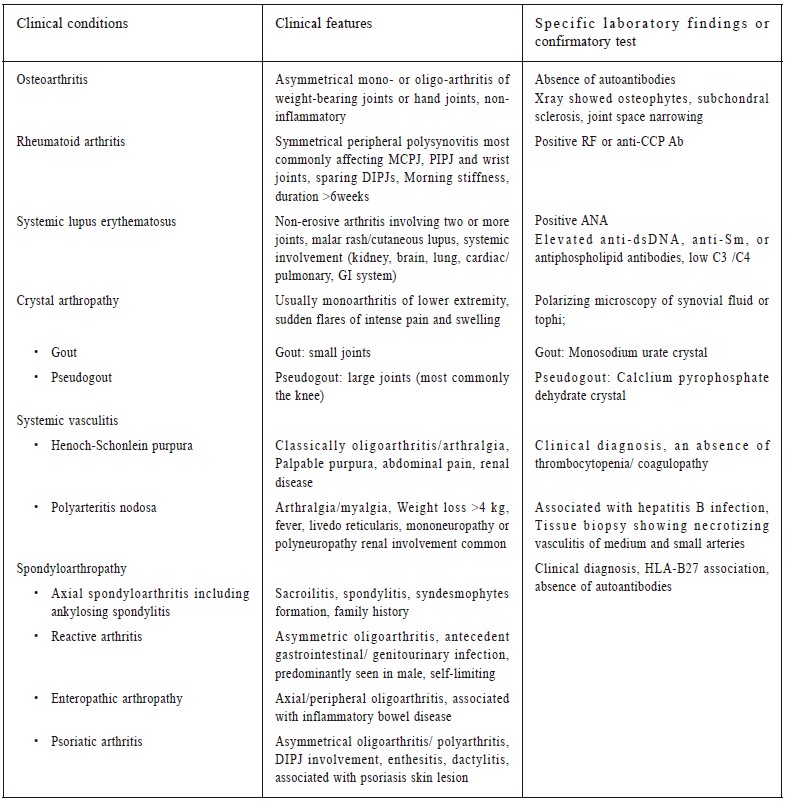
Table 2. Moll and Wright classification of psoriatic arthritis
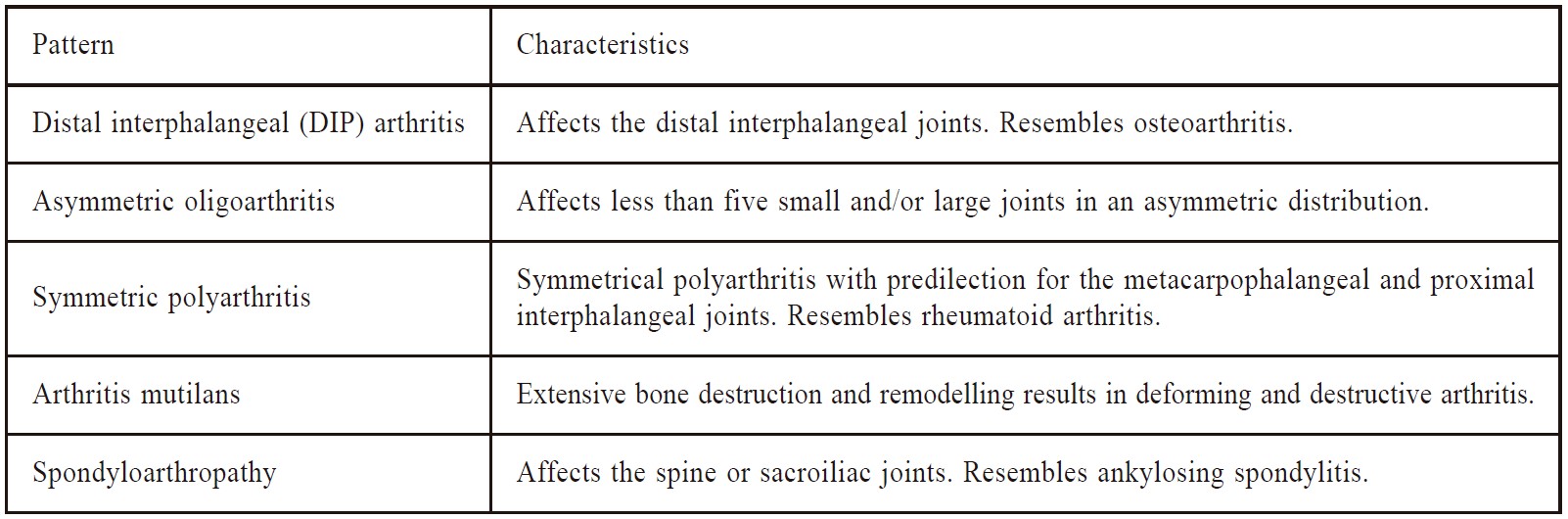
PsA typically develops between the ages of 30 and 50, but can arise at any age. In a cohort study carried out in Hong Kong in 2007, the mean age of onset of PsA was 38.8 (±11.8).4 In a recent study conducted in China, the prevalence of PsA in the Chinese population with psoriasis is about 10.4%.5 The psoriatic skin phenotypes associated with an increased risk of PsA were scalp lesions, nail dystrophy and intergluteal/ perianal lesions.6 In majority of PsA patients, the onset of arthritis was observed after a diagnosis of psoriasis. However, 7-15% of PsA patients may have arthritic symptoms before the appearance of any skin lesions.7 In these cases, a diagnosis of PsA can only be ascertained after the appearance of psoriatic skin lesion. However, a positive family history of psoriasis, specific joint features including enthesitis and dactylitis are more typical of PsA and these should alert family physicians to a possible case of PsA. As in our case, Mr. LKH presented with polyarthritis with subtle psoriatic skin lesions which were overlooked during the initial assessment. Therefore, it is essential for primary care physicians to actively inspect for skin psoriasis, nail changes and scalp lesions for all cases presenting with polyarthralgia. The clinical features of PsA are heterogenous. It may involve peripheral joints, axial joints, or both. Asymmetrical oligoarthritis is the most common joint pattern at disease onset.8 Enthesitis, tenosynovitis and dactylitis are common features. Classically, Moll and Wright characterized PsA into five patterns as summarized in Table 2.9 Diagnosis of PsA is essentially clinical, and should be a leading diagnostic consideration in any psoriatic patients with inflammatory arthritis in a pattern typical of PsA. Laboratory findings in PsA are nonspecific. Most common findings are elevated active phase reactants, sedimentation rate and leukocytosis, reflecting a nonspecific inflammatory response. There are no laboratory findings that are characteristic of PsA and can distinguish it from other forms of inflammatory arthritis or autoimmune rheumatic diseases. Historically, seronegativity for RF was required for the diagnosis. However, various studies have shown positive RF is present in 2 to 10% of patients diagnosed with PsA. As a result, the term “usually seronegative” arthritis is most suitable for PsA.10 Despite a lack of diagnostic tests, family physicians should increase the awareness of this diagnosis, as early diagnosis and treatment leads to improved long term outcomes. On the other hand, it is clearly demonstrated in studies, a delay in diagnosis of PsA of 6 to 12 months have been shown to be associated with joint damage and poor functional outcomes.11-13 The clinical course of PsA is variable. Some patients have only mild disease while others may suffer from severe erosive arthropathy associated with significant functional disability. The specific treatment for PsA depends on the severity and the type of psoriatic arthritis. A treat-to-target approach should be employed for peripheral and axial arthritis, with a target of remission or attaining minimal disease activity. For mild disease without joint damage, the first line of medication is NSAIDs. In patients whose peripheral arthritis remains active despite the use of NSAIDs, a conventional DMARD, usually methotrexate, is suggested. In patients presenting with severe erosive disease with functional limitation, a TNF inhibitor has to be introduced early in the course of the disease. For patients who are resistant to TNF inhibitors treatment, newer biologic agents targeting interleukin-17 and interleukin-23 are also available nowadays.14 With the launch of new biologic agents for psoriatic diseases in recent years, an early accurate diagnosis of PsA is paramount. Key messages
Non-pharmacological management strategies are just as essential in the treatment of PsA, and include physical and occupational therapy, exercise, prescription of orthotics, and education on joint protection. Weight reduction improves treatment response to DMARDs and biologic agents15 and overweight patients should be encouraged to attain their optimal body weight. Management of the increased cardiovascular risk factors and other comorbidities associated with psoriasis are also crucial. As such, family physicians play an important role in liasing with rheumatologists to offer holistic care to patients suffering from PsA. For our case, Mr. LKH presented with severe polyarthralgia with functional impairment, a more proactive approach with an early introduction of DMARDs including methotrexate and TNF inhibitor were adopted to bring his disease under control. He also continued his care in our department to date and has been also referred to our dietetic and physiotherapy departments for diet and weight reduction advice, and co-cared with the hospital rheumatologist. ConclusionPolyarthritis is a common clinical condition. Patients with psoriatic arthritis can present with polyarthritis without a known history of psoriasis. A systemic approach to rule out other inflammatory or rheumatoid diseases and careful inspection to identify psoriatic plaques or nail changes can lead to a timely and accurate diagnosis of psoriatic arthritis in primary care. References
Dr. Pui-kwan Chan,
MbChB, FHKCFP, FRACGP, FHKAM (Family Medicine)
Dr. Derek GC Ying,
LMCHK, FRACGP, FHKAM (Family Medicine)
Dr. Catherine XR Chen,
MRCP (UK), PhD (MED, HKU) , FRACGP, FHKAM (Family Medicine)
Correspondence to:
Dr. Pui-kwan Chan, Department of Family Medicine & General
|
|