
|
December 2025,Volume 47, No.4
|
Original Article
|
An audit on the management of diabetic vascular complication risk factors in a general outpatient clinic during the COVID-19 pandemicNelson Leung 梁景昭,Matthew MH Luk 陸文熹,David VK Chao 周偉強 HK Pract 2025;47:94-102
SummaryObjective: To evaluate the management of vascular complication risk factors in patients with Type 2 diabetes mellitus (T2DM) in a Hospital Authority (HA) General Out-Patient Clinic (GOPC) in Hong Kong during the COVID-19 pandemic, with the aim of improving the standards of clinical service provision.Design: The first phase of the audit, from 4/2021 to 3/2022, identified potential areas for improving the standards for managing vascular complication risk factors. The second phase of the audit, from 9/2022 to 9/2023, implemented improvement changes. The results of the two phases were compared. Subjects: All patients followed up regularly for T2DM at a GOPC. Main outcome measures: The key components necessary for the evaluation and management of vascular complication risk factors in T2DM patients were measured. Evaluation of vascular complication risk factors included ensuring that, at every clinic visit, blood pressure (BP) was measured, and at least annually, glycosylated haemoglobin (HbA1C), lipid profile, renal function, urine albumin-creatinine ratio (uACR), diet control, physical activity, body mass index (BMI) and smoking status were assessed for each patient. Management of vascular complication risk factors included ensuring that, unless contraindicated, a renin-angiotensin-aldosterone system inhibitor (RAAS-I) was appropriately prescribed, and that the individualised targets for HbA1C, BP and low-density lipoprotein cholesterol (LDL-C) were achieved for each patient. Results: Of the total 13 audit criteria, the target standard was achieved for 4 criteria in the first audit phase and 5 criteria in the second audit phase. In the second audit phase, raw improvement to standards were observed in 11 audit criteria, with 5 of these achieving statistical significance. Conclusions: A clinical audit with a targeted team approach to the implementation of changes achieved statistically significant improvements in the management of vascular complication risk factors in T2DM patients. Notably, these improvements were achieved despite significant HA GOPC service disruptions observed during the COVID-19 pandemic in Hong Kong. Keywords: Type 2 diabetes, vascular complication, Hong Kong, primary care, GOPC
摘要目的:評估香港醫院管理局(HA) 普通科門診診所(GOPC) 在COVID-19 疫情期間對第二型糖尿病(T2DM) 患者血管併 發症風險因素的治理情況,旨在提高臨床服務水準。設計:審計第一階段(2021年4月至2022年3月) 旨在確定血 管併發症風險因素治理的標準有待改進的領域。審計第二 階段(2022年9月至2023年9月) 旨在實施改善措施。兩個階 段的結果進行了比較。 對象:所有在GOPC 定期覆診的第2 型糖尿病患者。 主要結果測量:測量了治理2型糖尿病患者血管併發症風險 因素所需的關鍵指標。血管併發症風險因素的評估包括確 保每次門診就診時測量血壓(BP),並至少每年評估一次每 位患者的糖化血紅蛋白(HbA1C)、血脂狀況、腎功能、尿 液白蛋白-肌酸酐比(uACR)、飲食控制、體力活動、身體質量指數(BMI)和吸煙狀況。血管併發症風險因子的治理包括 確保除非有禁忌症,否則適當處方腎素-血管張力素-醛固 酮系統抑制劑(RAAS-I),並確保每位患者都達到HbA1C、 BP和低密度脂蛋白膽固醇(LDL-C)的個人化目標。 結果:在總共13 項審核標準中,第一階段審核中有4 項標 準達到了目標標準,第二階段審核中有5 項標準達到了目 標標準。在第二階段審核中,11 項審核標準得到了顯著提 高,其中5 項達到了統計學上顯著性差異。 結論:採用團隊方法實施有針對性改善的臨床審核,在2 型糖尿病患者血管併發症風險因素治理方面取得了統計學 上顯著的改善。值得注意的是,儘管香港在COVID-19 疫 情期間觀察到醫管局普通門診服務嚴重中斷,但這些改善 仍然能夠達成。 關鍵詞:家庭醫生,小型手術,基層醫療 BackgroundIn 2021, diabetes mellitus (DM) affected 537 million adults and was responsible for at least 966 billion USD in health care expenditure globally.1 In 2022, DM was the 11th commonest cause of death in Hong Kong with an estimated total prevalence of 8.5% amongst those aged 15 – 84, and according to a recent HA care report, amongst the 490,000 patients in Hong Kong that have their DM managed by the HA, twothirds were managed in the GOPC setting.2 Chan et al estimated that T2DM contributed up to 6.4% of the Hong Kong HA’s total expenditures for health care in 2004, and their retrospective cohort observational study found that the direct medical costs of T2DM increased significantly if complications were present, observing that patients suffering from either micro- or macrovascular complications and those suffering from both micro- and macro-vascular complications generated medical costs that were 1.1-fold and 1.3-fold higher than those patients without complications, respectively.3 Moreover, Wong et al observed that the costs of DM rise substantially in the years leading up to death.4 Since these studies were conducted, the HA published a care report reporting a 4.4% annual growth in DM prevalence between 2011 and 2020.2 These studies show the substantial and rising economic burden of DM and its associated vascular complications on the Hong Kong health care system. The benefits that may be achieved from effectively managing the risk factors of vascular complications in T2DM patients are undeniable, and the quality of care provided by GOPCs to this end is without question a relevant topic for evaluation. Lastly, as this audit was conducted amidst service disruptions caused by the COVID-19 pandemic, there was added interest to observe the effects of the pandemic on service provision and the resultant outcomes on vascular complication risk factor management in the GOPC setting, and to see whether audit interventions were able to raise standards of care despite these interruptions. Results of a pilot study on this topic at the authors’ GOPC, prior to the advent of service disruptions, are shown in Table 1, suggesting several areas for improvement. Objective and aimThe objective of this audit was to evaluate the process of care and the resultant outcomes in managing T2DM vascular complication risk factors in a GOPC, with the aim of achieving improvements in T2DM service provision:
MethodStudy designThis clinical audit consisted of 2 phases with comparable set-up and collection of data. The first phase of the audit, from 4/2021 to 3/2022, identified potential areas for improving the standards for managing vascular complication risk factors. The second phase of the audit, from 9/2022 to 9/2023, implemented improvement changes. The results of the two phases were compared, and evaluation of the effectiveness of the interventions was conducted. Specifically, medical records were reviewed to assess whether the following process and outcome audit criteria were achieved against standards informed and agreed upon after discussion with local colleagues and consideration of a recent HA DM care report, and these criteria are shown in Table 2.2 Table 1: Results of a pilot study on the management of vascular complication risk factors at the authors’ GOPC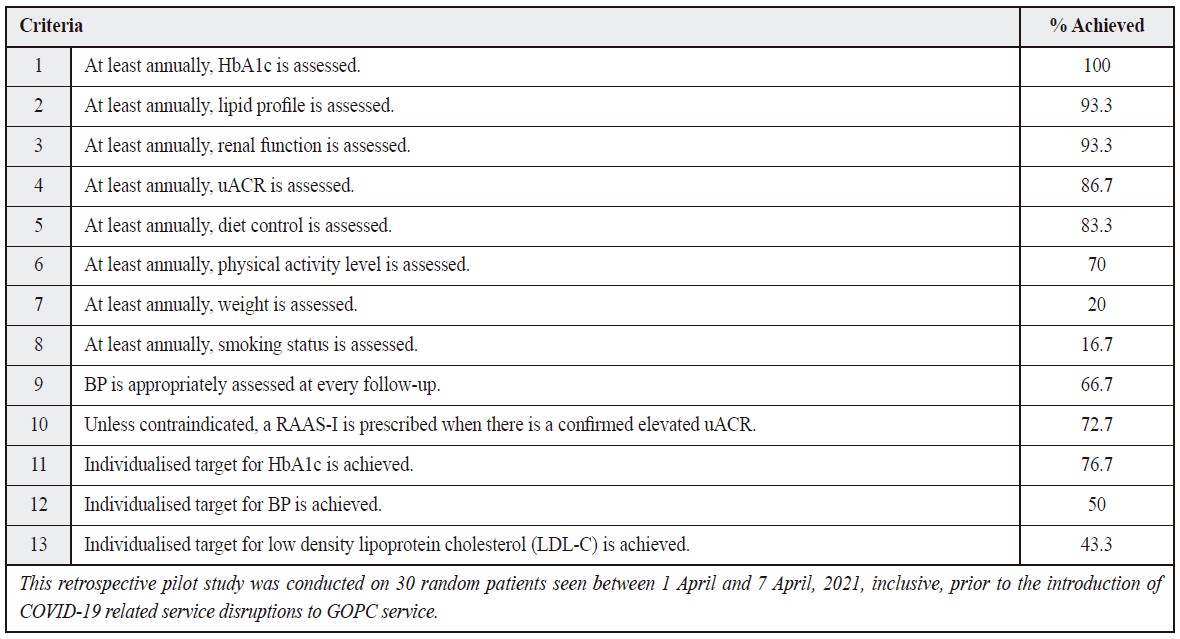
Table 2. Process and outcome audit criteria and agreed upon adult standards.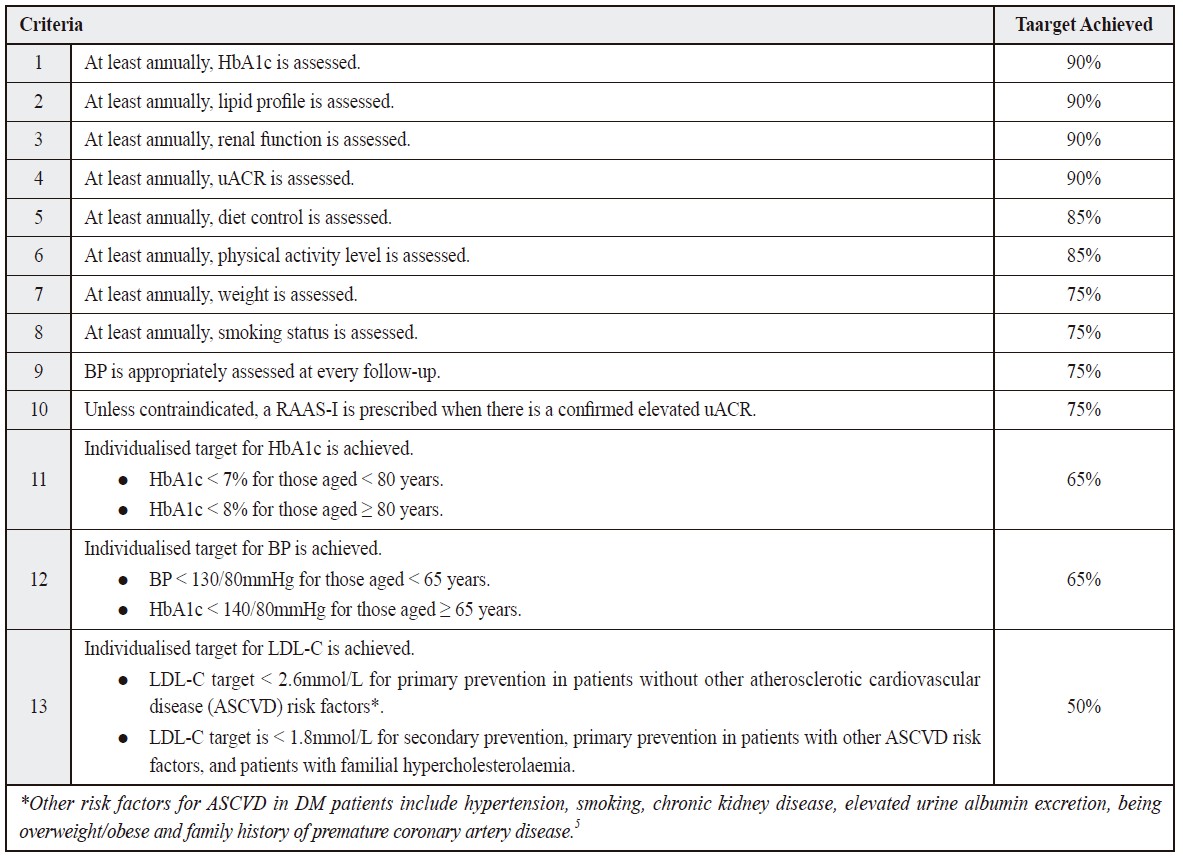
The evidence-based audit criteria and the setting of standardsTen process and three outcome criteria were assessed in this clinical audit. These were adapted from the local HA cluster’s Department of Family Medicine and Primary Health Care recommended criteria for auditing DM in GOPCs. The criteria were modified and added to after discussion with our GOPC’s clinic-in-charge and review of international, regional and local guidelines.5-7 Criteria 1 to 4 are relevant to the audit topic because they provide insight into a patient’s background vascular risk, which would inform clinical management. Chronic kidney disease (CKD), hyperglycaemia and hypercholesterolaemia are well-recognised vascular complication risk factors, and notable international, regional and local evidence-based guidelines recommend that HbA1c, lipid profile, renal function and uACR are assessed at least annually.5-7 Criteria 6 to 8 assess lifestyle habits that modify vascular complication risk and/or are themselves independent vascular complication risk factors. In terms of evidence, a healthy diet modifies vascular complication risk, and both the Dietary Approaches to Stop Hypertension (DASH) diet and Mediterranean diet patterns have been shown to produce positive effects on blood pressure, body weight, lipid profile and glucose metabolism, all of which are independent risk factors for vascular complications.8, 9 A multitude of studies have found that regular physical activity not only lowers cardiovascular and all-cause mortality risk, it also improves blood pressure, cholesterol control, glucose metabolism and lean body mass in patients with T2DM.10-13 Amongst DM patients, smokers have been observed to have worse glycaemic control and an increased risk of cardiovascular disease, microvascular complications, and premature death compared with those who do not smoke.14-16 Smoking cessation has been found to improve lipid profile as early as three weeks after quitting, and over the long-term, specifically reduces the risk of myocardial infarction, ischaemic stroke and diabetic nephropathy, with these benefits being more pronounced the younger the patient is at the time of quitting.16, 17 A recent study based on the EPIC-Potsdam cohort found that, after controlling for reverse causality and weight change secondary to disease severity and medical treatment, BMI reductions of more than 1% was associated with decreased risk for total microvascular complications, kidney disease and neuropathy compared to participants with a stable BMI.18 Optimising blood pressure and the use of RAAS-Is in T2DM patients with confirmed albuminuria reduces the risk of vascular complications, and criteria 9 and 10 help to achieve these outcomes. Blood pressure is another vascular complication risk factor, and multiple studies have shown that maintaining an optimal blood pressure reduces both cardiovascular events as well as microvascular complications.19, 20 In terms of criterion 11, a meta-analysis of 26 RCTs found that prescribing ACE-Is and ARBs in DM patients with confirmed albuminuria has been shown to reduce the risk of progressive chronic kidney disease, a major risk factor of cardiovascular disease.21, 22 It was felt that the standards for criteria 4 to 9 could be reasonably improved upon with reminders at small group discussion meetings and via electronic network communications and the creation of a DM consultation note template. For this reason, the standards were set at a higher level compared to those levels achieved in the pilot. The standard for criterion 10 was set similar to that achieved in the pilot because a substantial number of newly diagnosed albuminuria was not expected, and it was unlikely for patients with a history of albuminuria not to already have been prescribed RAAS-I therapy. With regards to criteria 11 to 13, suboptimal control of HbA1c, blood pressure and cholesterol are all risk factors for vascular complications, and as such, meeting the target levels for each of these parameters are clearly relevant for this audit. The targets stipulated for these criteria are supported by notable local, regional and international guidelines.6, 7, 23 Evidence from multiple trials suggests that HbA1c targets should be individualised. Specifically, major trials observed that intensive glycaemic control yielded no improved (ADVANCE), ambiguous (VADT) or even worsened (ACCORD trial) cardiovascular mortality alongside other risks of intensive glycaemic control.24-27 The findings were especially true amongst patients with a long duration of therapy, known history of hypoglycaemia and advanced atherosclerosis, suggesting that those of advanced age and frailty may benefit with less aggressive HbA1c targets (i.e. < 8%).28,29 The blood pressure targets of criterion 12 were obtained by multiple randomised controlled trials that have demonstrated that treatment of blood pressure to < 140/90mmHg reduces cardiovascular events as well as microvascular complications.19, 20 Additionally, the HOT study noted that an intensive diastolic blood pressure target of ≤ 80mmHg significantly reduced the risk of cardiovascular events by 51% in diabetic patients.,30 However, the ACCORD BP and SPRINT studies showed whilst aggressive systolic blood pressure targets < 120mmHg led to reduced risk of ASCVD, this benefit came at the cost of more adverse events from aggressive treatment, such as electrolyte abnormalities and acute kidney injury.31, 32 Last of all, the treatment of hypercholesterolaemia remains a contentious issue, with no overarching consensus amongst major international guidelines. Accordingly, the authors chose to base the LDL-C targets used for criterion 13 on regional and local guidelines.6, 7 Given that no DM-themed clinical audit was recently performed at this participating GOPC, the authors and local staff found it difficult to evaluate the reliability of the standards achieved in the pilot study. After comparison of the results against a recent 2019/2020 DM care report published by the HA, it seemed that the standards achieved in the pilot for the HbA1c target was likely an overestimation, whilst those achieved for the BP and LDL-C targets were reasonable approximations of the true situation.2 Nevertheless, it should be highlighted that the care report did not use the more stringent blood pressure and LDL-C targets this audit stipulated for certain patient subgroups, so whilst reasonably high standards of blood pressure and LDL-C control were reported, it is unclear how well these standards would fare against the overall more stringent targets this audit used.2 Subjects and sample size calculationIdentification and retrieval of all clinic patients coded with “T90 – Diabetes non-insulin dependent” under the International Coding for Primary Care 2nd edition (ICPC-2) was conducted using The Family Medicine module of the HA’s Clinical Management System (CMS).33 The study population sizes retrieved in such manner for phases 1 and 2 of the audit were 12,751 and 13,730, respectively. To obtain sample sizes to estimate proportions with a 95% confidence level and a 5% margin of error, the following formulae were used34, 35: 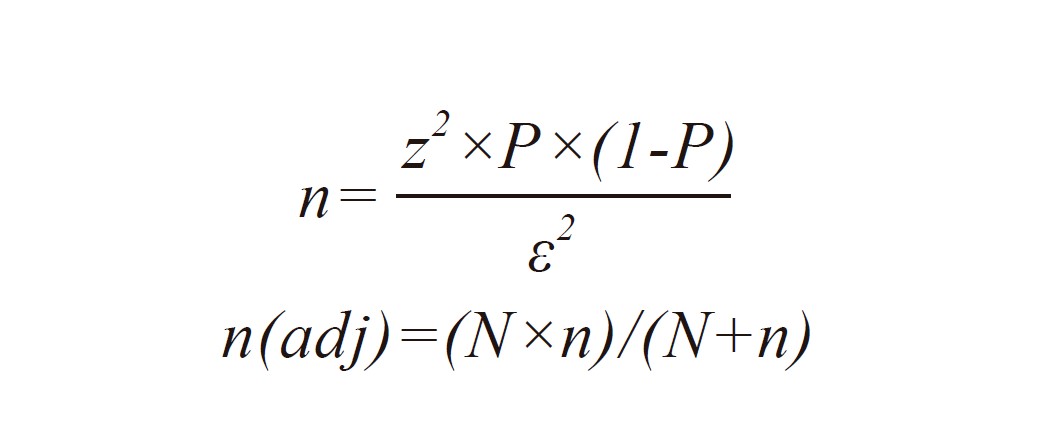
Where
z = Z-score = 1.96 P = Estimated true proportion = 0.5 ε = Margin of error = 0.05 n(adj) = Sample size adjusted for known population size N = Known population size The resulting sample sizes calculated in such manner for Phases 1 and 2 were 373 and 374, respectively. For each audit phase, the whole study population was randomised using the Microsoft Excel “RAND” function. The first 380 patients of the randomised study population list passing the exclusion criteria comprised the sample population for each audit phase. Exclusion criteria are shown in Table 3. Table 3. Exclusion criteria for the sample population for both phases of the audit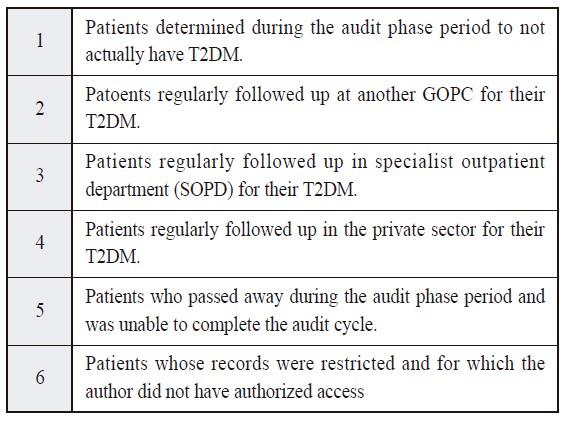
Data extraction and collectionThe computerised CMS medical records for the sample populations generated for each audit phase were retrieved by the principal investigator and reviewed against the 13 audit criteria for data collection. Outcome measuresThe main outcome measures refer to whether improvements were achieved in the audit criteria, and whether the results met the pre-set audit criteria standards. Statistical methodsAll statistical analyses for this audit were performed using the IBM® SPSS® Statistics software suite.36 With the normality of the age distributions of the sample populations for both audit phases confirmed by normal curves on histograms and normal Q-Q plots, the t-test for independent samples was used to compare the Phase 1 and 2 sample populations. Comparative analysis of the sex distributions and age group distributions between the sample populations were performed using the Pearson Chi-Square Test and the Fisher-Freeman- Halton Exact Test, respectively. All audit criteria outcomes were categorical variables, and the exact significance of the Pearson Chi-Square Test was used to identify statistically significant differences in all audit criteria outcomes between the pre- and post-intervention audit phases. InterventionsAudit interventions introduced to tackle the deficiencies in care identified in phase 1 of the audit were discussed and agreed upon with the participating GOPC doctors and other members of the health care team, and they are summarised in Table 4. Table 4. Audit interventions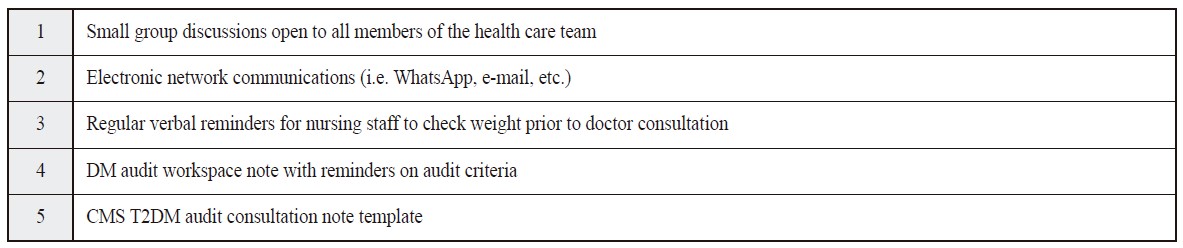
Table 5. Percent proportions of outcome criteria achieved against the target standards and the difference in outcomes between audit phases 1 and 2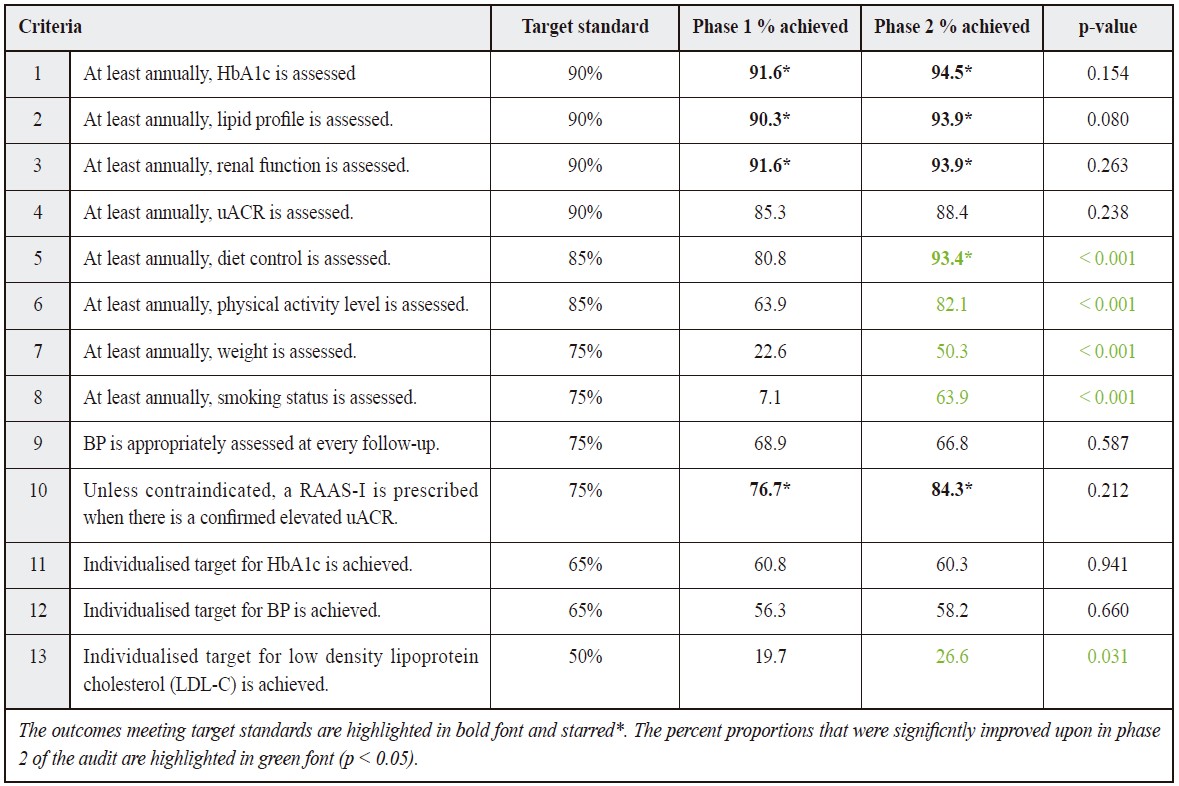
Small group discussions and electronic network communications served to update and remind clinic staff on audit criteria and recent clinical guidelines. Regular verbal reminders for nursing staff to check weight prior to the doctor consultation was specifically targeted at improving the poor standards achieved for annual weight assessment, and the DM audit workspace note was designed not only as an aid for GOPC doctors, but also as a means to introduce the audit efficiently to non-local, relieving-duty GOPC doctors who did not participate in the aforementioned, educational interventions. It was hoped that the Clinical Management System (CMS) T2DM consultation note template would help reinforce good medical record-keeping practice pragmatically and to help with time management. ResultsThe results of the outcome measures of both audit phases are summarised in Table 5. The sample populations of both phases are similar and comparable in terms of age and sex distribution. It is notable, however, that only patients of phase 2 were affected by the introduction of medication refill-only clinic sessions in response to the COVID-19 pandemic. As seen in Table 6, the number and percent proportion of sample patients affected by refill-only clinic sessions during the phase 2 collection period are 134 patients and 35.2%, respectively. Table 6. The number of refill-only clinic sessions attended by affected by patients.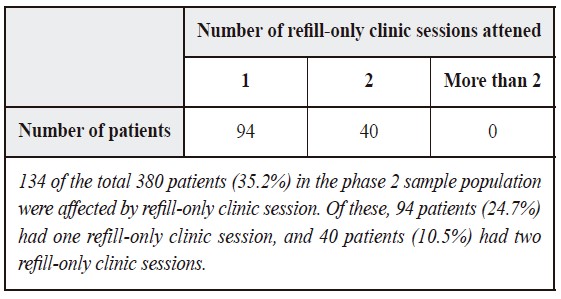
Of the total 13 audit criteria, the target standard was achieved in 4 criteria in phase 1 and 5 criteria in phase 2. In phase 2, improvements to standards were observed in 11 audit criteria; however, improvements to only 5 audit criteria - 5, 6, 7, 8 and 13 - were found to be statistically significant. Audit criteria 9 and 11 observed worsened outcomes in Phase 2, but neither of these were statistically significant. DiscussionWhat did this audit achieve?This audit identified areas of deficiency in the management of vascular complication risk factors in T2DM patients and provided convincing evidence of the types of baseline interventions that are effective at raising and maintaining these standards amidst service disruptions. Indeed, criteria 5 through 8 and 13 all experienced significant improvements in phase 2, and it was thought that the combination of educational small group discussions, verbal and written reminders and a CMS consultation note template accounted for these. This audit further raised the awareness of an important cornerstone of T2DM management - managing vascular complication risk factors - and reinforced good habits of maintaining adequate medical records and regularly advising patients on lifestyle modifications. The scale of disruptions by the COVID-19 pandemic was also reviewed in this audit. Why were some pre-set target standards not met?Reasons for deficiency in care and service provision may be classified into patient factors, doctor factors, team factors and systemic factors; these are summarised in Table 7, alongside ways to address them. In terms of patient factors, patients who are particularly frail or elderly, may not be ideal candidates for optimally tight blood pressure, HbA1c and LDL-C control, thereby affecting outcome achievement. Doctor factors that compromise care and service provision may include not being up-to-date with clinical management guidelines. Team factors include suboptimal communication between clinicians, nursing staff and health care assistants; it had been noted, for instance, that patients, whether by oversight or lack of reminders from clinicians, have not had their weights regularly assessed at follow-up, as evidenced by the fact that less than a quarter of patients had their weight assessed annually in phase 1 of the audit. In terms of systemic factors, for instance, as the study’s GOPC is open in the evenings and on public holidays, a proportion of T2DM patients would have had their condition followed up by clinicians not usually based at the said GOPC. These clinicians may have different, possibly looser DM management practices. Table 7. Summary of reasons for not meeting pre-set target standards and future interventions for consideration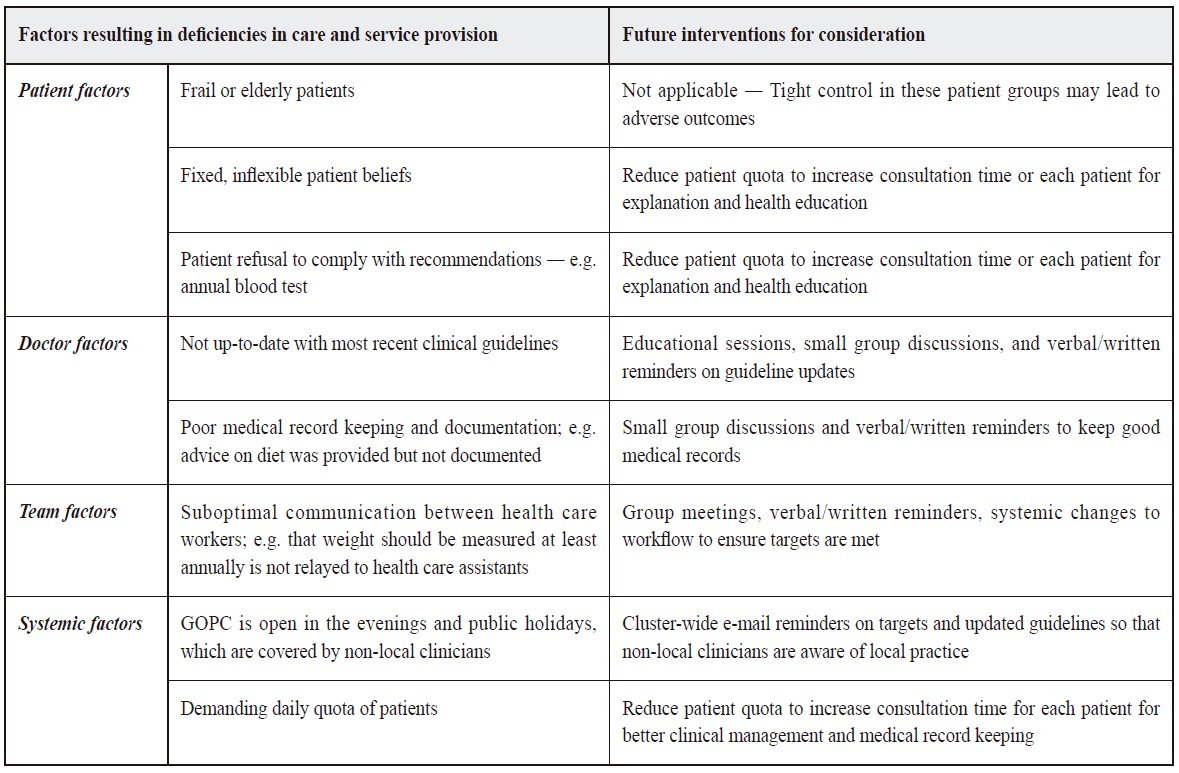
Service disruptions by the COVID-19 pandemic would have also impacted results. During phase 2, the regular follow-up period for stable chronic patients was changed from 16 weeks to 18 weeks commencing on 14/02/2023. Over a 1-year audit data collection period, this would translate into a patient seeing a doctor at follow-up only three times rather than four times previously. Refill-only clinic sessions, where a prescription would be issued to a stable patient without seeing the patient, were also implemented during the phase 2 data collection period. The overall reduction of routine patient contact during the COVID-19 pandemic would have compromised optimal care provision. LimitationsThe sample populations were not directly comparable because of pandemic-related service disruptions during the phase 2 data collection period; accordingly, a direct evaluation of the effectiveness of the audit interventions would be difficult. Notably, other parameters, such as home blood pressure monitoring and the self-monitoring of blood glucose, could be used as outcome measures, and future audits may incorporate these as audit criteria outcomes. Additionally, large population subsets, such as private patients or patients with more complex needs that are managed in the SOPD setting, were excluded from our study and were not evaluated. Future directionsExploring changes in patterns of drug prescribing between audit phases may provide further insight and be considered in future audits; indeed, it may have been insightful to consider whether - and if so, how - the usage of statin changed between the phases to account for the significantly improved outcome achieved for the LDL-C target. Other interventions, such as involving senior management to consider reducing daily consultation quota for increased patient contact time, loosening the limitations on the types of oral anti-diabetic medications that may be prescribed in the GOPC, and integrating patient-inputted data from mobile application platforms directly into computerised medical records for increased efficiency, could be considered in future audits on this topic. Collaboration with other GOPC units may also be considered. Key messages
AcknowledgementsThe authors would like to thank fellow colleagues for their advice, guidance and participation in this audit exercise. References
Nelson Leung,
MB ChB (Warwick), MRCSEd, MRCGP, FHKAM (Family Medicine)
Matthew MH Luk,
MB ChB (CUHK), FRACGP, FHKCFP, FHKAM (Family Medicine)
David VK Chao,
MB ChB (Liverpool), MFM (Monash), FRCGP, FHKAM (Family Medicine)
Correspondence to: Dr. Nelson Leung, Family Medicine and Primary Care Centre,
G/F, Li Shu Pui Block, Hong Kong Sanitorium and Hospital,
2 Village Road, Happy Valley,
|
|