
|
June 2022,Volume 44, No.2
|
Original Article
|
Patients’ sources, views and perceptions of drug information, and the relationship with drug compliance in a primary care settingTammy KW Tam 譚嘉渭,Dominic MW Lau 劉敏維,Kinson KS Lau 劉建生,Kwok-keung Ng 吳國強, Cecilia YM Fan 范婉雯 HK Pract 2022;44:37-50 Summary
Objective:
We examined patients’ sources, views and
perceptions of drug information and the relationship
with drug compliance in a primary care setting.
摘要
目的 :
研究基層醫療患者的藥物資訊來源,對藥物資訊的
看法和觀念以及與藥物服從性的關係。
關鍵詞 : 藥物,藥物依從性,基層醫療,患者 IntroductionMedication non-adherence is a major medical and public health concern globally. The World Health Organization defines medical adherence as “the extent to which a person's behaviour corresponds with agreed recommendations from a health care provider.”1 The reported rate of non- adherence varies widely in different studies from 10% to 92%.2 Among patients with chronic illness, approximately 50% do not take medications as prescribed.1 A large body of literature reveals that non-adherence in patients leads to poor therapeutic outcomes, substantial worsening of disease, higher patient mortality and increased health care costs.3-5 Medication-taking behaviour is complex and individual. It is the result of an interplay of numerous patient, physician, medication and health care systemrelated factors6,7 Obstacles to medication adherence include inadequate knowledge about a drug and its use, not being convinced of the need for treatment, fear of adverse effects of the drug, long term drug regimens, poly-pharmacy and complex drug regimens.8 On the other hand, providing useful prescription information to improve understanding of drug treatment is an important way to ensure optimal medication use.9-11 A quantitative survey revealed that, despite more easy access to health information using internet, health professionals are still regarded as the most reliable sources of drug information.12 Besides, the quality of information and how patients perceive them constitute other important determinants for the eventual medication-taking behaviour.13 The primary objective of this study was to investigate patients’ sources of drug information and how patients perceived the usefulness of the information. As drug compliance can have a s significant impact on the outcome of chronic illnesses, we would investigate how the perception of drug information would affect drug compliance with chronic medications. We hope the results would inform clinicians in pursuing strategies for effective delivery of drug information as a way to optimise the use of medications, hence promoting a better health outcomes for patients. MethodsThis was a cross sectional study conducted by means of a questionnaire survey. It was approved by the Ethics Committee of the Department of Health, HKSAR on 4 July 2018. We conducted the study in six primary care (outpatient) clinics among sampled subjects aged 18 or above who had attended the clinic for a medical consultation during a period from 3 September 2018 to 29 March 2019. Daily patient appointment record in each clinic would form a list for sample selection each day during the study period. Each appointment record contained the number of appointment slots equivalent to the number of available quotas for that day. Each appointment slot was numbered. In selecting subjects, three numbers from each clinic were identified each day using the random number table. The corresponding subject in the appointment slot would be recruited for the study. Trained counter staff would invite them to participate in the study upon their presentation at the reception counter. If the subject was below the age of 18, the one in the next appointment slot would be invited. No substitution would be arranged for subjects who refused to participate. A self-administered questionnaire in Chinese or English where appropriate, was distributed to the sampled subjects by the counter staff. Nurses taking charge of the study was responsible for collecting the questionnaires upon its completion. If necessary, they would also assist with questionnaire completion. For subjects with special needs such as hearing and speech difficulties or for those who could not communicate in Cantonese, Putonghua or English, assistance from their accompanying household members/caregivers to facilitate completion of this study was allowed. All sampled subjects were, at the beginning of the interview, informed of the nature and purpose of the survey, voluntary participation, and anonymity as well as confidentiality of information collected. They were asked to give verbal consent before proceeding and were informed that agreement to or decline to participating in this study did not affect the services provided to them by the clinic. The questionnaire consisted of 33 questions (Annexes), which covered demographics (Q1-7), healthseeking pattern (Q8-9), medical illnesses (Q10), drug compliance rate (Q11), sources of drug information (Q16), views (Q12-15, Q17-18, Q32-33) and perception of drug information, e.g. easy to understand or not, useful or not (Q19-31). Subjects were encouraged to answer all questions relevant to them. There were instructions on the questionnaire to guide subjects on how to skip a certain question(s) if not relevant to them and to continue with the remaining questions. For example, if they did not have any illnesses that would require regular follow up / treatment, they were asked to skip question 10 and go directly to question 11 after question 9. In data analysis, the base number for each question was generated according to the actual number of responses to that question. Take question 10 as an example, which asked whether one had any chronic illnesses, 762 out of 2,165 subjects had skipped that question as they did not have chronic illnesses; the base number for that question would be 1,403. A series of quality control measures were adopted to ensure that all data collected from the study would be of satisfactory quality. Training before the study, and further training sessions during the study if necessary, were arranged to provide solutions to the difficulties encountered by the counter staff and nurses. Nurses would check the questionnaire completed by the participants for its completeness and dubious responses to individual questions such as gender or age mismatch, if any. Clarification with the participants would be made on the spot once such dubious entries were identified. Furthermore, about 15% of the questionnaires would be checked against the corresponding data inputted into the computer. The questionnaires were anonymous. All questionnaires filled with data and data files were regarded as confidential documents, and the study team would exercise due care in its handling. All the data collected from the study was used for research and statistical purposes only. All questionnaires filled with respondents’ information would be destroyed within six months after completion of the survey. Statistical analysisIt was proposed to enumerate a random sample of patients, after balancing the level of precision of estimates required, the resources and time constraints. Taken response rate of 90% based on previous studies with a similar design performed by our team 14, the proposed sample size of 2,300 was considered adequate to achieve a precision level with an estimated sampling error within ±5 percentage points with a 95% confidence level. As for data analysis, descriptive analysis was performed for all questions. Pearson’s Chi-squared test or Fisher’s exact test (if expected cell count was less than 5), would be performed to evaluate the association between the reported drug compliance rate and other relevant independent variables pertaining to demographics (Q1-7), views (Q12-15, Q32) and perception of drug information (Q19-31). Logistic regression analysis would be performed to adjust the confounding effect between variables. P-value <0.05 was regarded as statistically significant. ResultsDuring the study period, a total of 2,365 subjects were invited, 2,165 agreed and returned the questionnaires, giving the response rate of 91.5%. The base number for each question was generated according to the actual number of responses to that question. Missing data were excluded from analysis, they accounted for <1% of all responses. The base number would be stated if it was different from 2,165. Among the participants, 47% (1,018) were males, and 71.4% (1,546) were aged above 50 years. About half of the participants (50.3%, 1,088/2,161) were working at the time of study. Among the non-working population, majority of them (67.8%, 725/1,070) were retired, followed by housewife (30.0%, 321/1,070), unemployed (1.4%, 15/1,070), student (0.6%, 6/1,070), and others (0.3%, 3/1,070). As for education level, 49.8% (1,077/2,161) completed secondary education and 40.7% (879/2,161) attained tertiary education or above. Table 1 showed the socio-demographic variables of the subjects. About participants’ health-seeking behaviour, 86.7% (1,874/2,162) would seek doctor’s advice when feeling unwell, 37.7% (814/2,162) would consume over-the-counter western medications and 24.0% (518/2,162) would seek Chinese practitioners’ advice. As for the frequency of seeing doctors, 64.9% (1,404/2,163) visited the doctor at least 4 times per year, and 13.8% (298/2,163) more than 10 times per year. About their health status, 63.6% (1,378/2,165) had at least one chronic illness that required regular follow up, mostly hypertension (58.4%, 805/1,378), followed by hyperlipidaemia (22.2%, 306/1,378) and diabetes mellitus (21.1%, 291/1,378). 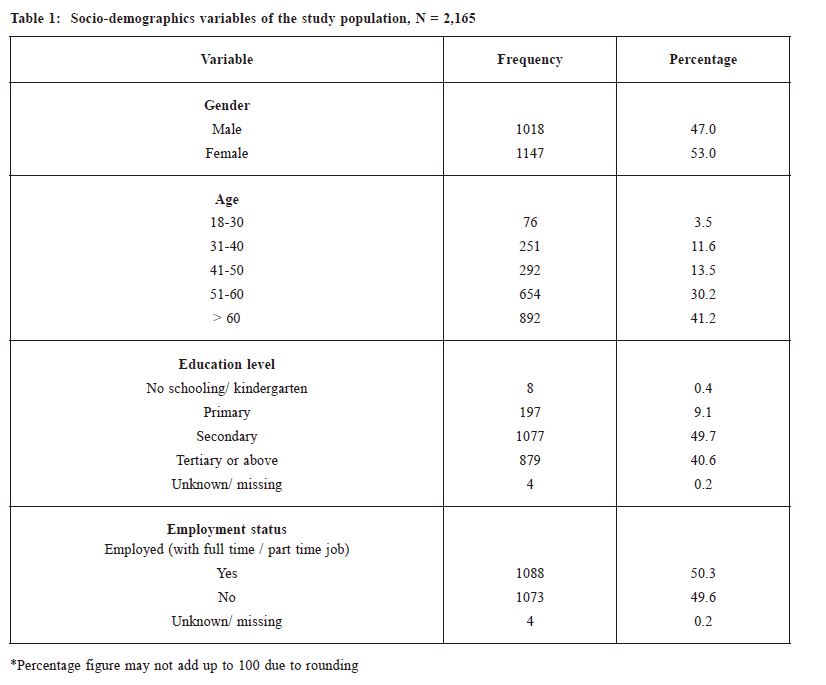
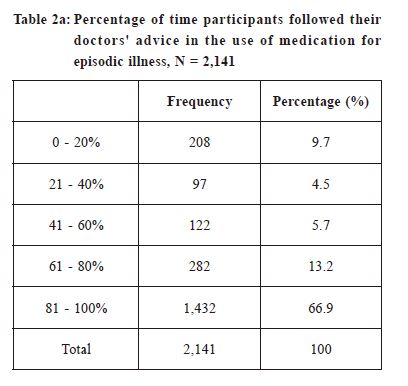
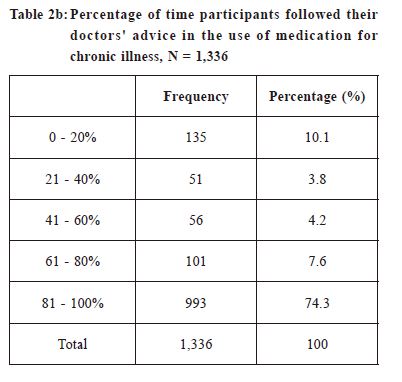
Regarding the views on drug information, 91.9% (1,985/2,160) strongly agreed/ agreed that drug information is necessary, and 90.7% (1,959/2,160) strongly agreed/agreed that provision of drug information makes one more likely to use medications according to doctor’s advice. On the other hand, 73.0% (1,576/2,160) strongly agreed/ agreed that information about untowards effects of drugs would adversely affect their drug-taking decision. As for the source of drug information, 81.5% (1,757/2,156) regarded doctors as the most important source of information to them, followed by pharmacists/ dispensers (47.8%, 1,030/2,156), drug information leaflets in clinic (32.4%, 699/2,156), and nurses (20.5%, 443/2,156). Besides, 17.3% (372/2,156) of subjects regarded the internet as the most important source of drug information. About the type of drug information that was considered most important, 80.2% (1,722/2,147) were concerned about side effects of medications, followed by 56.1% (1,205/2,147) about how to administer the drug and 41.9% (899/2,147) about drug efficacy. About the type of medications that most concerned them, 73.5% (1,587/2,158) were about antibiotics, 66.0% (1,425/2,158) about steroids, and 54.8% (1,183/2,158) about chronic medications. When given drug information leaflet, only 37.7% (814/2,158) would always/ often read it. For those who had read the drug leaflet, 64.3% (1,215/1,889) strongly agreed/ agreed that it is easy to understand and 82.4% (1,556/1,889) strongly agreed/ agreed that it is useful. Logistic regression showed there was statistically significant association between reading drug information leaflet and good drug compliance (81-100%) for episodic illnesses (p = 0.000; OR 1.88, 95% CI 1.27-2.78). During doctor’s consultation, 10.6% (228/2,147) were always given drug information, 21.8% (467/2,147) often, 52.2% (1,120/2,147) sometimes and 15.5% (332/2,147) were never given drug information. If given drug information by doctors, 80.8% (1,473/1,824) strongly agreed/ agreed that it is easy to understand, and 90.2% (1,646/1,825) strongly agreed/ agreed that it is useful. During drug collection, 70.7% (1,527/2,159) strongly agreed/ agreed that drug information given by pharmacists/ dispensers is adequate, 75.4% (1,627/2,158) strongly agreed/ agreed that the information is easy to understand, and 83.2% (1,796/2,158) strongly agreed/ agreed that it is useful. Regarding the frequency of searching drug information by internet, 16.4% (355/2,161) always/ often searched internet for drug information, 53.0% (1,146/2,161) sometimes did so and 30.5% (660/2,161) never did so. For those who had searched internet for drug information, 36.0% (539/1,499) strongly agreed/ agreed that it is reliable, 54.8% (822/1,499) were neutral, and 9.2% (138/1,499) disagreed/ strongly disagreed it is reliable. As for whether the internet information is useful or not, 52.9% (793/1,500) strongly agreed/ agreed that it is useful, and 44.3% (665/1,500) is neutral and 2.8% (42/1,500) disagreed/ strongly disagreed it is useful. Having received different drug information from other sources, 58.4% (1,261/2,159) of subjects would continue to adhere to doctor’s advice in taking the medications, 40.1% (865/2,159) would sometimes stop the medications, and 1.5% (33/2,159) would always/ often stop taking it. We define good drug compliance as 81-100% adherence to the doctors’ recommendations. Overall, 66.9% (1,432/2,141) reported good drug compliance in episodic illnesses (Table 2a), and 74.3% (993/1,336) in chronic illnesses (Table2b). For analysis of drug compliance rate in chronic illnesses, logistic regression showed good drug compliance was associated with tertiary education (p = 0.007, OR 2.17, 95% CI 1.28-3.69) often/always received drug information during clinic visit (p = 0.000; OR 2.08, 95% CI 1.22-3.54 and OR 6.09, 95% CI 2.37-15.63 respectively), and agreement that drug information improves medication- taking behaviour (p = 0.027, OR 1.90, 95% CI 1.08-3.35) (Table 3). On the other hand, the drug compliance rate was not shown to be associated with the perception of whether or not drug information received was useful or easy to understand (Table 4). Regarding the internet as a source of drug information, there were no statistically significant associations between drug compliance and frequency of searching the internet, or perceptions whether or not the internet is true and reliable, easy to understand or useful. 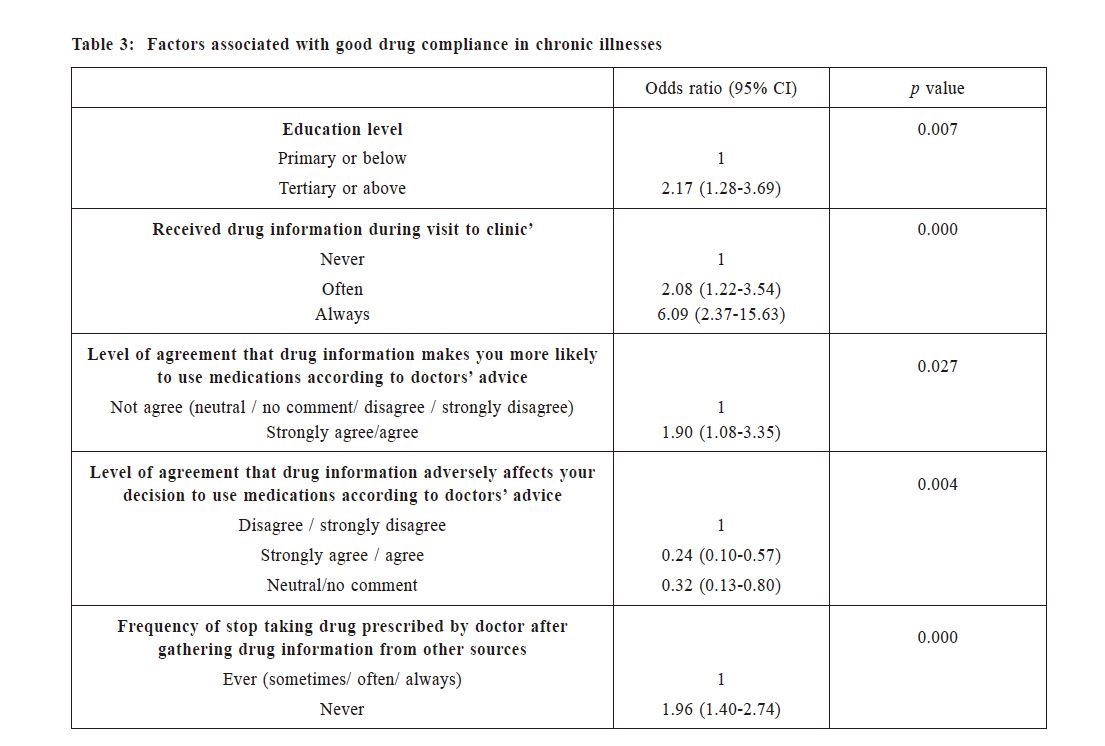
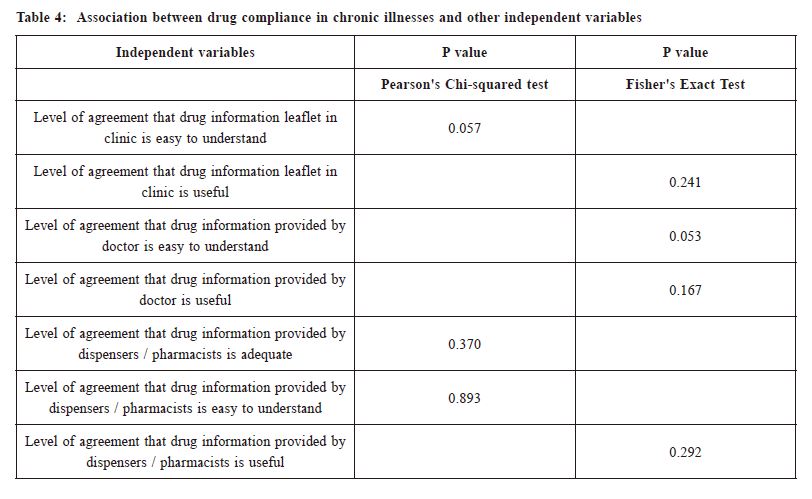
DiscussionThe study recruited 2,165 subjects from 6 clinics over 7 months. By analysing data collected from selfadministered questionnaires, we examined patients’ sources of drug information, views and perceptions of drug information and the relationship with drug compliance.We found that there was a strong agreement that drug information is important in improving patients’ compliance to prescribed drug treatment. Doctors were far regarded as the most important source of drug information, and the information was perceived with the highest rate of understandability and usefulness when compared with pharmacists/ dispensers, drug information leaflets, nurses and internet. Our findings were similar to a quantitative survey which revealed that, despite more easy access to health information using internet, health professionals are still regarded as the most reliable sources of drug information.12 Doctors, being the most reliable and trustful source of drug information to patients, however, were not able to deliver drug information at every consultation. Our results showed that only 32.4% of subjects always or often received drug information from doctors during consultation. One of the reasons might be time limitations. The participating clinics provided both episodic and chronic care. The average consultation time for each patient was around 5-10 minutes. Doctors often had to manage multiple problems with different degrees of complexity within a single consultation session. Therefore, drug information might be more often given to those patients with special needs such as elders, pregnant women, etc, or when prescribing special groups of medications such as antibiotics and steroids. It is encouraging that when given drug information by doctors, most subjects were able to understand and found them useful. Distribution of preset drug leaflets in consultation might be a practical way to enable doctors to deliver drug information in a busy practice. It is intriguing that although drug leaflet was regarded as the third important source of drug information and were generally regarded as easy to understand and useful, only 37.7% would always/ often read them if they were available in clinic. When we examined the health-seeking pattern of participants, we found that 65% of them visited doctor at least 4 times per year, and 14% even more than 10 times per year. It might be possible that subjects had repeatedly come across the same set of drug information leaflets in clinic over the year. Besides, 64% of participants had at least one chronic illness that required regular follow up. They might already be using the medications for quite some time. The accumulated knowledge and experience with the use of these medications might diminish their interest in reading drug leaflets. As echoed by other studies, patients’ needs and quest for information will change over time in response to their personal experiences with the medications.15 Drug information leaflets might need to cover a wide range of different medications, particularly those most concerned e.g. antibiotics, steroids, and chronic medications. They have to be updated regularly to keep abreast of new developments and knowledge and in keeping with the needs, preferences, and drug use experience of people. The widespread use of the internet as an information source has aroused active concerns from health professionals.16,17 It has been reported that 80% of adult internet users have accessed it for general health information and 36% of them specifically for medication information.18 It is noteworthy that the highly variable and uncontrolled quality of health information in the world wide web has been shown to cause adverse outcomes.17 Similarly, 70% of our subjects would at least sometimes searched the internet for drug information. Fortunately, only one-third of them believed the information was reliable and the perception of the usefulness of internet information was much lower than that provided by doctors’, pharmacists’/dispensers’ or drug information leaflets’. The reason might be the participants were generally more mature. Seventy percent of them were above 50 years old and over 90% had attained secondary education or above. The overall rate of good drug compliance was 66.9% for episodic illnesses and 74.3% for chronic illnesses. Our analysis was more focused on chronic illnesses because optimal control of which is tied to improved health outcomes, better survival benefits, and a more cost-effective health care system.3-5 For participants who agreed that drug information has bearing on drug adherence, their drug compliance in chronic illnesses was already better than those who did not. Furthermore, those having received drug information were found to be strongly associated with good drug compliance. Interestingly, we found no significant relationship between drug compliance and the perception of whether the drug information was understandable or useful or not. It was more the act of receiving drug information from trustful persons, than the process of understanding that had made the difference in medication-taking behaviour. This was in line with the findings that drug compliance was found not associated with the habit of internet searching or perception of internet information in this studied population. Overall, our study suggested more effort should focus on strategies to enable doctors to deliver drug information, which should also be targeted and relevant to the needs of an individual patient. As regards the limitations of the study, the questionnaire used was not properly validated, though the process of design did go through repeated cycles of evaluation and verification by a group of doctors, pharmacists and statisticians so as to envelop the most relevant dimensions of the concept under study. The questions about drug compliance should be based on more validated tools for measuring drug compliance. The mean age of our subjects was above 50 years. Most of them had attained secondary education or above. The overall characteristics might not be the same as the Hong Kong population at large. Therefore, the findings might not be generalisable to all clinic settings. The median age of the Hong Kong population is around 45 years. Our population has ease of access to health education through different means via public and social media. Our results might be a meaningful reference to other settings as well.
ConclusionDoctor was regarded as the most important source of drug information. The information provided was perceived as easy to understand and useful. Though the internet was a common way for searching drug information, the perception of its usefulness was the lowest. What most concerned patients were the side effects of medications, how to administer the drug and drug efficacy, particularly those pertaining to antibiotics, steroids, and chronic medications. Good drug compliance was strongly associated with the provision of drug information, regardless of whether the information was perceived as understandable or useful or not.
AcknowledgementsWe are indebted to colleagues in the Health Statistics Division, Department of Health for their tremendous support in the design of the questionnaires and data analysis of this study. We also thank every doctor, nurse and clerical colleague in the Team who were involved in coordinating and conducting data collection. Their perseverance and dedicated effort have contributed greatly to the success and publication of this study.
References
|
|