
|
June 2022,Volume 44, No.2
|
Case Report
|
A case report on atypical angina: assessment of chest pain in primary care settingTak-kei Tse 謝德基,Catherine XR Chen 陳曉瑞 HK Pract 2022;44:59-63
SummaryCoronary artery disease (CAD) is one of leading causes of disease burden and of death. Diagnosing CAD is sometimes difficult as few patients present with typical features of angina. Delayed diagnosis can have potentially serious consequences. Here we report a case of CAD, presented in primary care with atypical angina.
摘要冠心病是一種可致命及成為長期病患的重要疾病。因 只有少數患者呈現典型心絞痛徵狀,在診斷時,有時也會 遇上困難。延誤診斷會引起嚴重的潛在後果。本文彙報一 宗在基層診所出現的非典型心絞痛病例。
IntroductionHeart disease is prevalent in Hong Kong (HK). According to statistics from the Department of Health (DH), heart disease was the third leading cause of death in HK, accounting for 12.5% of all death in 2019.1 Among the different types of heart diseases, coronary artery disease (CAD) is the commonest and accounted for 66.6% of all deaths caused by heart disease in 2015.2 The prevalence of CAD in HK increases over the years, likely due to the ageing population, presently escalating burden of chronic diseases, and the sedentary lifestyles of life.3Chest pain is one of the most common presentations encountered in primary care and making a diagnosis can be challenging. Despite most cases of pain are noncardiac and benign in nature, it is the family physicians’ responsibility to pick up imminent cases of serious heart disease. Study found that 27.0% of patients with acute coronary syndrome (ACS) had visited the primary care in the preceding 30 days and up to 11.0% were missed and not referred for hospital care on those visits.4 In light of this, we report a case which presented with atypical chest pain in general practice and discussed the approach for proper assessment and identification of CAD in the primary care.
The CaseA 46-year-old gentleman, who is a chronic smoker and non-drinker, had been regularly followed-up at a General Out-Patient Clinic (GOPD) of the Hospital Authority of Hong Kong (HAHK) for management of hypertension (HT) and type 2 diabetes (T2DM) for 8 years.
HistoryOur patient had consulted several general practitioners in both private and public sector for chest and shoulder pain and was treated as having musculoskeletal (MSK) pain. Despite the use of analgesics and home exercise, the pain remained unchanged.He described the chest pain as dull in nature, intermittent and lasted for 5 to 10 minutes each time. Every time, the pain was precipitated by lifting heavy weights at work and was relieved by rest. The chest pain did not occur when he walked upstairs or upslope. As his job was already labour-intensive, he did not have extra exercise. The last episode of chest pain was 5 days ago. Other than the pain, there was no nausea or vomiting, no sweating, no palpitation, no shortness of breath nor orthopnoea. There was no history of injury to his body anywhere. To give further clarification of his shoulder pain, he revealed that he had suffered from shoulder pain since six months earlier and the pain had no temporal relationship with the onset of his present chest pain.
Physical examinationOn Physical examination(PE), his general condition was satisfactory. Body mass index (BMI) was 30.2 kg/m2, clinic Blood pressure (BP) was 128/67 mmHg and heart rate (HR) was 68/min, regular.Musculoskeletal examination (MSK) found no obvious bony deformity. There was mild tenderness over both acromioclavicular joints with reduced range of movement on cross-body adduction. Cardiac assessment was unremarkable, with no audible murmurs. There were no signs of heart failure with normal breathing sounds and no lower limb ankle oedema.
InvestigationX-ray of chest and shoulders had been performed in private before, both were unremarkable.Office electrocardiogram (ECG) (see Figure 1) was done and showed sinus rhythm with Q wave in V1 and T-wave inversion in II, III, aVF, V5-V6. There were no acute ST-segment changes. Possibility of concomitant acromioclavicular osteoarthritis with stable angina was explained to the patient in view that the chest pain was associated with high level of exertion (i.e. lifting heavy objects), in addition, he had an abnormal baseline ECG and other cardiovascular risk factors including chronic smoker, obesity, sedentary lifestyle and comorbidities with T2DM and HT. The patient then proceeded with computerised tomography coronary angiography (CTA) with contrast in the private sector and the report showed 70% stenosis of right coronary artery (RCA), with 30% stenosis over proximal left anterior descending artery (LAD) and left circumflex artery (LCx). Aspirin and statin were started immediately, and he was referred to the cardiac team urgently for further management. At the same time, the patient was referred to the nurses for smoking cessation counselling, and diet and lifestyle modifications for body weight control. 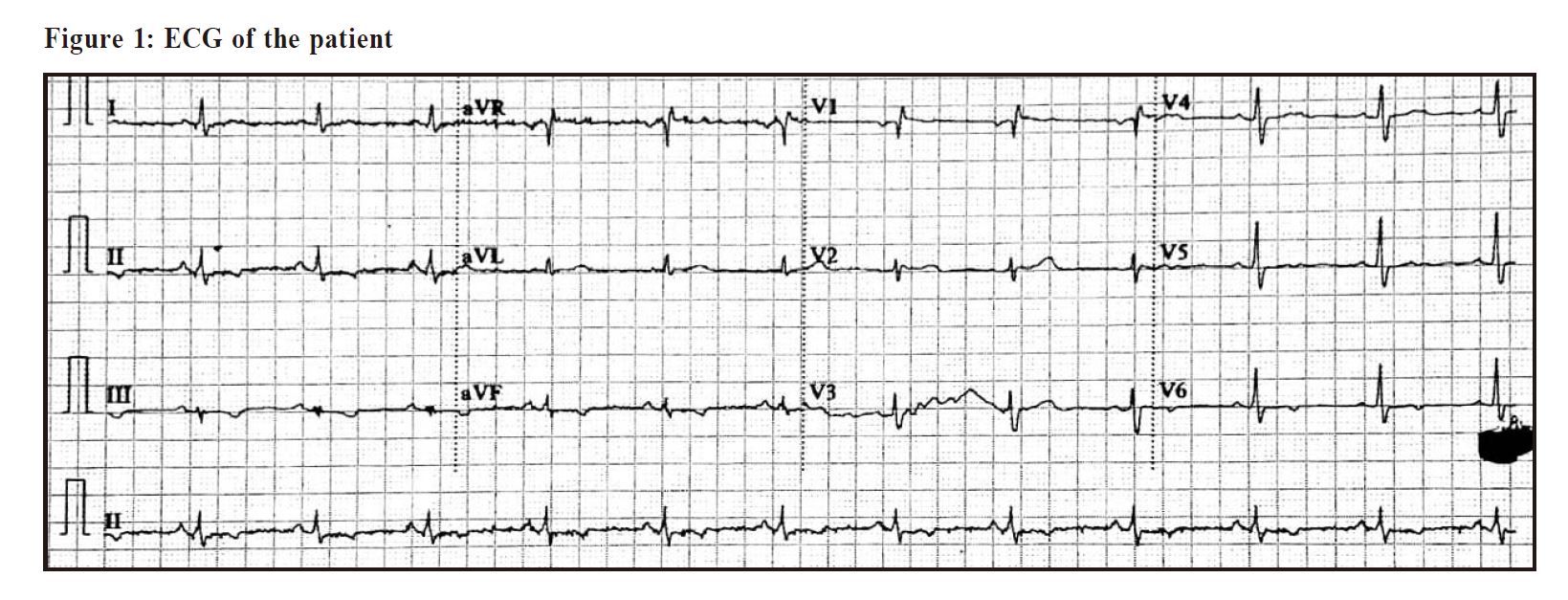
DiscussionChest pain is a common complaint presenting to primary care physicians. Picking up potentially lethal cases is often challenging. Patients with chest pain due to ischaemic aetiology often appear to look well. As such, the initial diagnostic approach should always be to consider a cardiac aetiology, unless other causes are apparent. A focused history and physical examination will define high-risk patients and a baseline ECG is the “key” immediate investigation primary care physicians must obtain.The first decision point for most physicians is whether the chest pain is caused by coronary ischemia. Clinical characteristics associated with an increased likelihood of ACS include male sex plus age over 60-years; diaphoresis; pain that radiates to the shoulder, neck, or jaw; and past history of angina or ACS.5 Our patient suffered from atypical chest pain which occurred only when he lifted heavy objects and was not aggravated by other physical activities. This history might indicate the pain to be MSK in origin. Indeed, studies have shown that most patients suspected of having CAD present with atypical or non-angina chest pain, only as few as 10-15% present with classic symptom of severe or crushing central chest pain exacerbated by exertion and relieved by rest.6 The differential diagnoses for chest pain are diverse.9 Although most common causes of chest pain in the primary care population include chest wall pain (20%), reflux esophagitis (13%) and costochondritis (13%)10, other life-threatening causes should not be missed (Table 1). One prospective cohort study identified four clinical factors that predict a final diagnosis of chest wall pain: localised muscle tension, stinging pain, pain reproducible by palpation, and the absence of a cough.11 Burning retrosternal pain, acid regurgitation, sour or bitter taste in the mouth will support the diagnosis of gastroesophageal reflux disease. 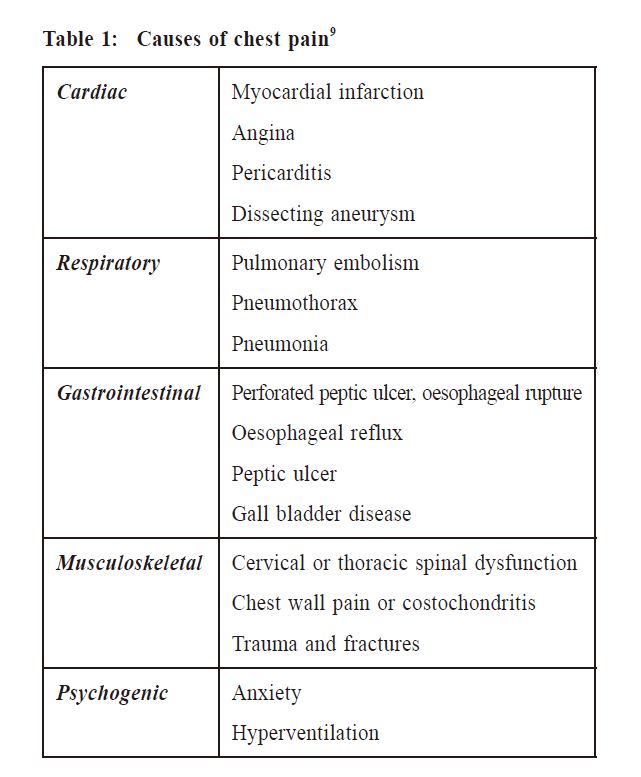
The initial goal in the management at outpatient setting is to determine whether the patient needs further testing such as troponin I or cardiac imaging test for ACS. The NICE guideline12 and ESC guideline6 have detailed algorithms on the assessment and diagnosis of recent onset chest pain of suspected cardiac origin. Firstly, we need to determine whether the patient is having acute chest pain or stable chest pain. Symptoms and signs that may indicate an ACS include (i) current chest pain lasting longer than 15 minutes, (ii) chest pain in past 12 hours with abnormal ECG, (iii) chest pain associated with nausea and vomiting, marked sweating, breathlessness, (iv) pain with haemodynamic instability, (v) new onset chest pain or abrupt deterioration in patients with known stable angina. These patients should be referred to the hospital or to cardiologist for urgent same-day assessment. As our case did not have symptoms suggestive of ACS and the last episode of chest pain occurred 5 days ago, it is reasonable to manage him in the outpatient setting. For patients with suspected stable angina as with our case, detailed history and careful PE should be carried out to identify cardiovascular risk factors.13 Indeed, optimisation of cardiovascular risk factor modification is always an integral component of patient care in our daily practice. Our patient had multiple cardiovascular risk factors and therefore concerted effort should be made to ensure that all these are under good control. Resting 12-lead ECG should be performed for the evaluation of all cases of chest pain, including atypical and non-anginal pain. Although normal resting ECG does not rule out stable angina, certain changes may indicate ischaemia or previous infraction. It includes pathological Q-waves, new onset left bundle branch block, ST-segment and T-wave abnormalities (flattening or inversion).14 In our case, the baseline ECG showed Q-wave and T-wave inversion. Although there was no previous ECG for comparison, these findings should prompt for further cardiac investigation. Concerning the appropriate diagnostic tests for obstructive CAD, both functional and anatomical noninvasive tests can be considered.6,12 Common functional tests include stress cardiac magnetic resonance and stress echocardiography. Anatomical non-invasive evaluation refers to CTA. In the latest update of NICE guideline in 201612, CTA is recommended as first line investigation for (i) typical or atypical angina or (ii) non-angina chest pain but resting 12-lead ECG indicates ST-T changes or Q-waves. To detect obstructive CAD at both thresholds of 50% and 70% stenoses, CTA can achieve sensitivity of 95-99%, specificity of 64-83% and a negative predictive value of 97-99%.15,16 Furthermore, the 2019 the European Society of Cardiology (ESC) guideline6 also recommended the use of CTA as first line investigation for patients with a lower range of clinical likelihood of CAD. Significant CAD is defined as ≥70% diameter stenosis of at least one major epicardial artery segment or ≥50% diameter stenosis in the left main coronary artery. For our case, due to the limited resources and long waiting time for CTA in HAHK (more than 1 year), our patient had private CTA done and the report showed severe stenosis with ≥70% diameter stenosis over RCA with mild non-obstructing CAD over proximal LAD and LCx. Therefore, the case was referred to the cardiac team urgently for consideration of percutaneous coronary intervention. 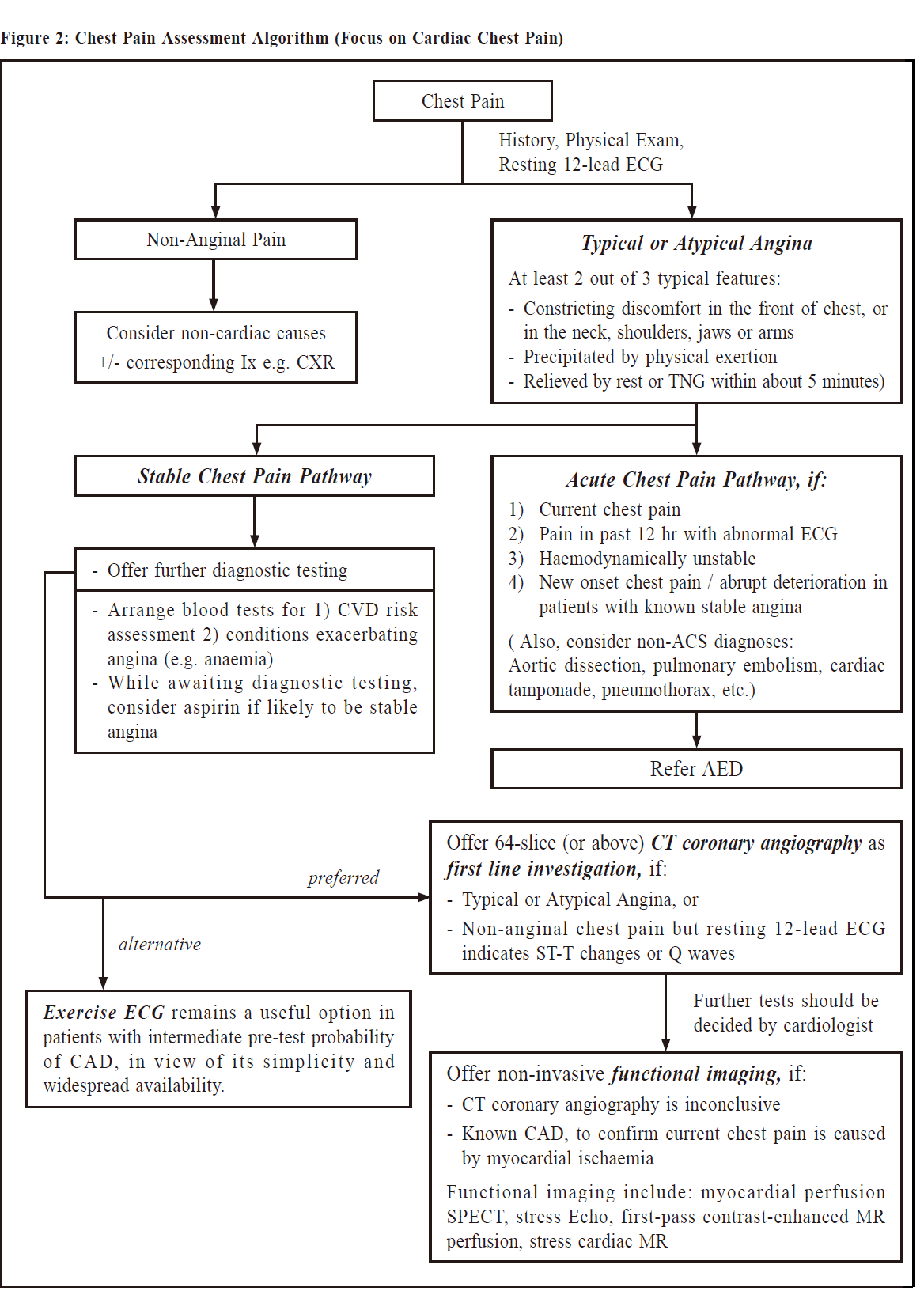
In the past, exercise ECG was recommended as one of the first line tests. Nowadays it has a limited role due to its inferior diagnostic performance to rule-in or rule-out obstructive CAD (sensitivity of 46-69% and specificity of 54-69%).17 Also, exercise ECG is not useful in patients with pre-existing ECG abnormalities (such as left bundle branch block, paced rhythm, Wolff- Parkinson-White syndrome, ≥0.1 mV ST-segment depression on resting ECG) that prevent interpretation of the ST-segment changes during stress, or in patients unfit for high-level exercise.6 However, it may still be considered as an alternative if other tests are not available.6 Therefore, family physicians should advise the pros and cons of different cardiac tests to patients thoroughly and the choice should be individualised according to patient’s risk and preference and the availability of the tests. A flow chart on chest pain assessment as modified from the NICE guideline12 and ESC guideline6 is shown in Figure 2. For patients with stable angina, lifestyle modification and optimal medical therapy is the key for reducing symptoms, stopping progression of atherosclerosis, and preventing major adverse cardiovascular events. Revascularisation is always as an adjunct to medical therapy instead of replacing it6, but the indication and choice of revascularisation are beyond the scope of this article. Referencess
Tak-kei Tse, MBBS (HK), FRACGP, FHKCFP, FHKAM (Family Medicine)
Catherine XR Chen, MRCP(UK), PhD (Medicine, HKU), FRACGP, FHKAM (Family Medicine)
Correspondence to: Tak-kei Tse, Yau Ma Tei Jockey Club General Out-patient Clinic, |
|