|
June 2016, Volume 38, No. 2
|
Discussion Paper
|
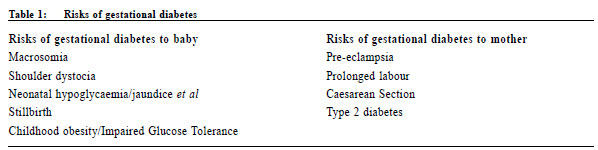
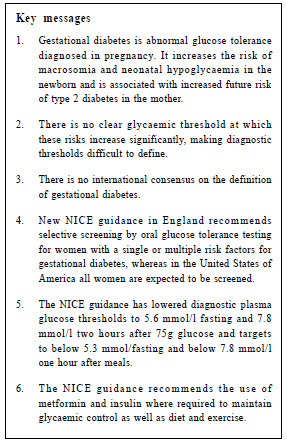
The evolving management of gestational diabetesMary Charlton HK Pract 2016;38:53-59 Summary Gestational diabetes has been recognised since the days of RD Lawrence when he wrote his book “The Diabetic Life” in the 1920s. It is an abnormality of glucose tolerance diagnosed in pregnancy that is of sufficient severity to increase the risks of foetal macrosomia and neonatal hypoglycaemia and associated with increased future risk of type 2 diabetes in the mother. The condition is hard to define because there is no clear glycaemic threshold at which these risks increase and there is no international consensus. New National Institute of Health and Care Excellence (NICE) guidelines in England recommend selective testing by oral glucose tolerance test for pregnant women with a single or multiple risk factors for gestational diabetes, whereas in the United States of America all women are expected to be screened. The NICE guidance has lowered diagnostic plasma glucose thresholds to 5.6 mmol/l fasting and 7.8 mmol/l two hours after 75g glucose, and targets to below 5.3 mmol/l fasting and below 7.8 mmol/l one hour after meals. It recommends the use of diet and exercise to maintain glycaemic control and metformin and insulin where required. Timing of delivery is determined by the complexity of the case but may be as late as 40+6 weeks’ gestation in straight forward situations. Postnatal follow-up and management with diet, weight management and exercise are crucial in the prevention of future maternal diabetes. 摘要 上世紀20年代,在RD Lawrence撰寫《糖尿病人的生活》一 書後,妊娠糖尿一症受到確認。它是在妊娠期間出現的糖耐量異常,而其程度足以增加巨大胎兒和新生兒低血糖症 的風險,亦會增加該孕婦未來罹患2型糖尿病的機會。然而妊娠糖尿的定義,難以設訂。原因是並沒有一個明確令風 險增加的血糖閾值,而國際上對此也未有共識。最新的英國NICE指引建議選擇性地,只對呈現一項或多項 妊娠糖尿風險因素的孕婦進行口服葡萄糖耐量試驗檢測,而美國則建議對所有孕婦進行篩查。N I C E指引已將空腹 血糖診斷閾值降低至5.6mmol/l和75g葡萄糖後2小時的血糖閾值定為7.8 mmol/l;而把空腹時的目標血糖水平定為 5.3 mmol/l以下和餐後1小時值定在7.8 mmol/l以下。該指引同時建議利用飲食和運動方法來控制血糖,並在需要時使 用二甲雙胍和胰島素。 分娩時間會按個別案例的複雜性而決定。情況簡單的,也 可延至妊娠40+6周。產後訪視、飲食管理、體重管理和運 動,都對產婦預防未來罹患糖尿非常重要。 lntroduction Last year saw the publication of new guidelines issued by NICE on the diagnosis and management of Gestational Diabetes (GDM) in the National Health Service (NHS) in England and Wales.1 Now, then, is an opportunity to review how attitudes and evidence have shaped the approach to GDM over the previous decades and to look at the new NICE guidance on GDM. Twentieth century approaches to gestational diabetes Soon after the arrival of insulin injection, one of its earliest beneficiaries2, Dr RD Lawrence, wrote of diabetes in pregnancy in his book “The Diabetic Life”3: “The prognosis and outlook depend chiefly on whether the diabetes develops during pregnancy or whether pregnancy occurs in a diabetic.” This statement has stood the tests of time and statistics. Although pregnancy outcomes in women with type 1 and type 2 diabetes are now better than when Lawrence first wrote these words4, pre-existing diabetes remains associated with far more complications for the mother and baby than does GDM.5 For decades, this difference was so great that the need to treat gestational diabetes or not at all was controversial.6 Although Lawrence did not use the term gestational diabetes, he went on to describe the typical resolution after delivery, and likely recurrence of diabetes in subsequent pregnancies. He recommended treatment with “qualitative” carbohydrate restriction augmented, if necessary, by insulin. He also published a case report dramatically illustrating the hazards of transient diabetes in pregnancy.2 The woman in question had five successful pregnancies apparently uncomplicated by GDM, followed by another 6 pregnancies each with diabetes, 5 culminating in stillbirths and 1 live birth of a baby weighing 5.7kg. Following the last and final of her 11 pregnancies, her diabetes “disappeared”! Lawrence’s sad account is, fortunately, not one we might expect to encounter today but it illustrates well some of the complications of gestational diabetes (Table 1). Gestational diabetes The term “gestational diabetes” was initially used
to describe women with a poor obstetric history who,
during a subsequent pregnancy, had high glucose levels on oral glucose tolerance tests.7 Following a United
States of America recommendation that gestational
diabetes should be recognised as a distinct entity8
criteria for diagnosis were drawn up in 1980 by the
American Diabetes Association involving a two step
procedure for all pregnant women9:
In 1999, the World Health Organisation defined GDM as: “Any degree of glucose intolerance first recognised in pregnancy:
“The diagnostic criteria for hyperglycaemia in pregnancy recommended by the World Health Organisation (WHO) in 1999 were not evidence-based”.13
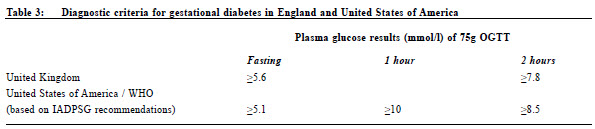
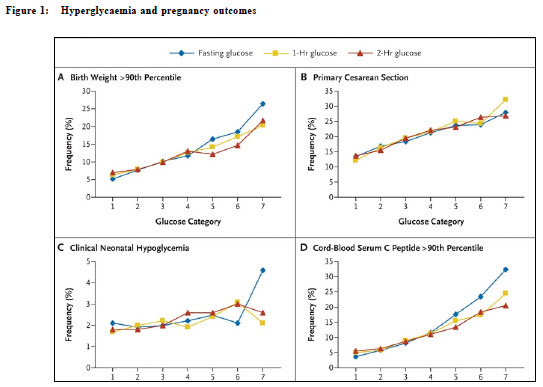
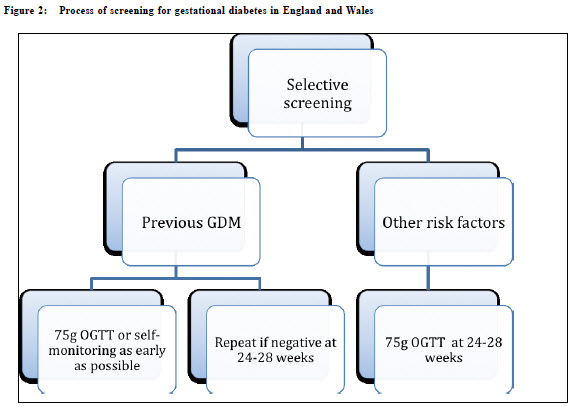
Into the new millennium The controversies around GDM have included whether GDM should be defined by adverse foetal or maternal outcomes; whether all women should be screened or only selected “higher risk” women or none at all; which tests were appropriate for screening and diagnosis, and what thresholds were considered abnormal. Indeed, there is an opinion that it should not be given a disease status but to be seen as a risk factor for macrosomia.7 Into this vacuum came a well-conducted multinational randomised controlled trial, the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS). Most authorities have accepted its conclusion that intensive treatment of Gestational Diabetes reduced risk of serious perinatal complications from 4% to 1%.14 The WHO criteria remained unsatisfactory, based as they were on the non-pregnant state. In 2008, the Hyperglycaemia and Pregnancy Outcomes (HAPO) study15 (Figure 1) showed no obvious maternal glucose levels at which any of its studied outcomes became noticeably more frequent, thus the medical community was left with good evidence that there is a continuum of risks related to a continuum of maternal glycaemia but without clear-cut diagnostic criteria. What was clear, however, is that fasting glucose level was of greater significance than had previously been realised. In 2010, the International Association of Diabetes and Pregnancy Study Group (IADPSG), comprising a body of clinicians and statisticians, looked further into HAPO data16, and recommended that high risk women should be tested for pre-existing diabetes in early pregnancy and there should be universal screening at 24 weeks pregnancy with the 75g OGTT. Compared with WHO 1999, the fasting level for diagnosis was lowered to 5.1 and the 2 hour level raised to 8.5 (Table 3). The 2015 guidance from the National Institute For Health and Care Excellence (NG3) Screening for gestational diabetes NICE’s new guidance, NG3, retains a selective, rather than universal, approach to screening for GDM (Figure 2). Risk factors are listed as a BMI above 30 kg/m2; a previous macrosomic baby weighing 4.5 kg or above; previous gestational diabetes; a family history of diabetes in a first degree relative and/or an ethnic family origin with a high prevalence of diabetes. A woman with one or more risk factors is to be offered a 75g OGTT at 24-28 weeks gestation unless she has had GDM in a previous pregnancy. In this latter case she should be tested in early pregnancy with either an OGTT or self-monitored blood glucose (SMBG). This will identify women who have developed type 2 diabetes or impaired glucose tolerance and enable early and appropriate management. If early testing is normal, OGTT or SMBG should be repeated at 24-28 weeks. Diagnostic criteria for GDM After re-evaluating the IADPSG criteria for diagnosing GDM in light of published evidence and the NHS health economy, NICE recommends the following as GDM diagnostic thresholds using the 75g Oral Glucose Tolerance Test: Fasting plasma glucose ≥ 5.6 mmol/l These are simpler than, although not the same as, IADPSG recommendations (Table 3).
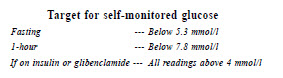
Management of GDM There are some practical organisational recommendations on GDM management in NG3. These include: consultation in a joint antenatal diabetic service (run by obstetric and medical specialists together) within a week of diagnosis; dietary advice on a low glycaemic index diet from a dietitian and taking 30 minutes’ exercise after meals; prompt communication with primary care doctors and measuring HbA1c to identify those who may have pre-existing type 2 diabetes. Additional to routine antenatal monitoring is ultrasound assessment of foetal growth and amniotic fluid volume every 4 weeks from 28 to 36 weeks. Education and equipment should be given to enable SMBG with the following targets:
Initial treatment is with lifestyle modification, and when these targets are not met, medication is introduced. If ultrasound suggests macrosomia or polyhydramnios or fasting glucose is 7 mmol/l or more, then insulin is introduced at once. In the United Kingdom, the use of metformin in pregnancy has been widely accepted from the time of the Metformin in Gestational Diabetes (MiG) study.17 It has the obvious advantage of being, given orally which is simpler and less painful for women, rather than by injection. It results in less maternal weight gain which should improve postnatal glucose tolerance. Concerns about it crossing the placenta were largely allayed by the MiG outcomes. In more than 40% of women, metformin is likely to require supplementation with insulin as pregnancy progresses.1 Glibenclamide, in contrast, has not found much favour in GDM mangement. The dose required to control post-prandial glucose puts women at risk of pre-meal hypoglycaemia and it is less flexible than insulin in terms of mealtimes and diurnal glycaemic variation. Presumably unavailable to the compilers of NG3 were the results of a systematic review in the British Medical Journal.18 The poorer outcomes for both mother and baby when glibenclamide was used make it even less likely that glibenclamide will be routinely used.
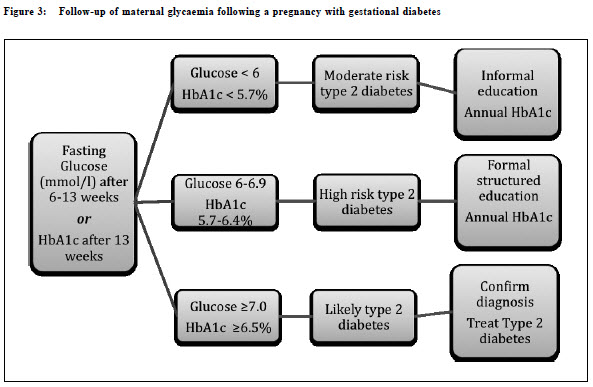
Insulin, when required, is introduced in a “basal plus” regimen, tailored to the woman’s glycaemic profile. Fasting hyperglycaemia is treated with a basal insulin, usually NPH insulin. Postprandial hyperglycaemia is treated with mealtime doses of a rapid-acting analogue insulin used according to post-meal SMBG relevant to each meal. So a woman may need no insulin, one dose or a full basal-bolus multiple dose insulin regimen. All antidiabetic medication is withdrawn at delivery (except in the rare situation of suspected new-onset type 1 diabetes in pregnancy). Birth In the past, NICE guidance did not offer advice on timing of delivery in GDM as distinct from type 1 or type 2 diabetes. This meant that most women with GDM were delivered between 38 and 40 weeks’ gestation. The new guidance gives greater flexibility, recommending that women with GDM to give birth no later than 40+6 weeks, but earlier if there are maternal or foetal complications. Delivery should be in hospital with neonatology facilities and maternal blood glucose should be checked every hour during labour and maintained between 4 and 7 mmol/l. Postnatal management of women following GDM When a woman with GDM gives birth, her insulin and metformin are stopped immediately. It is expected that her random glucose will be checked before discharge from hospital and that she will be given advice on reducing her risk of future GDM, and indeed type 2 diabetes, through diet, weight management and exercise. Postnatal testing The use of an OGTT to establish a mother ’s diabetic status following delivery is no longer recommended. Instead, a fasting glucose should be checked at postnatal follow-up which, in the UK, is usually around 6 weeks following childbirth. If this opportunity to check at 6 weeks is missed, then HbA1c becomes useful 13 weeks following delivery. The interpretation of results and consequent stratified action is in line with previous NICE guidance on prevention and diagnosis of diabetes.19 (Figure 3) Conclusion Although the significance of transient hyperglycaemia during pregnancy has been recognised since the early days of diabetic medicine, the definition of gestational diabetes and its management have been evolving as evidence emerged. New guidance on the management of gestational diabetes in England and Wales, NG3, issued by NICE, has set diagnostic criteria: a fasting plasma glucose of 5.6 mmol/l or above, or a 2 hour plasma glucose of 7.8 mmol/l or above on 75g Oral Glucose Tolerance Testing. Management is diet, exercise, blood glucose and foetal growth monitoring, combined obstetric and diabetic medicine care, metformin and insulin. Timing of delivery is determined by the complexity of the case but may be allowed in straight forward situations to reach 40+6 weeks’ gestation. Postnatal follow-up and management with diet, weight management and exercise is crucial in the prevention of subsequent maternal diabetes.
Mary Charlton, BSc, MBBS, MRCP
Specialty doctor in diabetes
Correspondence to: Dr Mary Charlton, Diabetes Centre, Nuffield House, University
Hospital Birmingham, Birmingham B15 2TH, United Kingdom.
References
|
|