|
March 2007, Volume 29, No. 3
|
Update Articles
|
The importance of the primary dentition to children - Part 2: effects of treating carious teeth by extractionNigel M King, Robert P Anthonappa, Anut Itthagarun HK Pract 2007;29:101-107 Summary The short-term consequences of dental caries in primary teeth include pain and infection. Early management of carious lesions in children can prevent such sequelae, lessen the trauma to parents, save costs and time and to provide better quality of oral health. An important function of the primary teeth is to maintain the natural dental arch and to allow the permanent teeth to erupt in an orderly fashion with adequate space. If carious lesions are not treated early, extraction will be the only treatment option, which in turn, depending on the age may have adverse effects on the developing permanent dentition. Children with severe dental caries usually require the extraction of several and, on occasions, all primary teeth. Premature loss of primary teeth by extraction will influence the occlusal relationship and space in the permanent dentition. Children like to have a set of teeth similar to those of their peers and thus avoid ridicule and criticism. Any criticism directed at a child's missing, or unsightly teeth may be traumatic to his/her psychological development. Therefore, carious primary teeth should not be left untreated until extraction becomes the only treatment option. Several restorative approaches and materials are available to restore the primary teeth. However, restorative management of carious teeth is only the first phase of treatment and its success lies in maintaining a favourable oral environment. Therefore, treatment should be definitive yet specific for each individual child, with long term follow-ups and reinforcement of preventive measures. 摘要 乳齒齲病在短期間可引致痛楚和細菌感染等嚴重後果。及早診治兒童齲病可預防這些後遺症,減輕對父母造成的創傷, 節省金錢和時間,以及使口腔更加健康。乳齒的其中一個重要功能是維持正常的牙弓,好讓恆齒有足夠空間整齊地長出。 如果未能及早治療齲病,拔牙將是唯一的選擇,視乎兒童的年齡,拔牙可能會對恆齒生長構成不良後果。當患上嚴重齲病, 兒童需要拔掉多顆甚至全部乳齒。拔牙引致的乳齒過早脫落是會影響將來恆齒的嚙合關係和生長空間。孩子喜歡擁有一副和朋輩一樣的牙齒, 以免受到嘲笑和批評。對孩子缺牙或不美觀的各種批評,會對其心理成長造成創傷,所以,不要讓齲病的乳齒留待到非拔牙不可時才加以治療。 多種修護方法和物料可用於修補乳齒。為齲病修復只是治療的第一步,它的成功有賴於經常保持良好的口腔狀況, 所以對個別兒童的治療必須明確和具體,而且需要長期覆診和強調各種預防措施。 Introduction The primary teeth play a critical role in the growth and development of a child. In addition to their roles in aesthetics, eating, speech, and to encourage normal function and expected growth, the other main function of the primary teeth is to provide space for their permanent successors and until the permanent teeth are ready to erupt. Without the primary teeth, the permanent successors cannot assume their proper position in the dental arch. The short-term consequences of leaving dental caries in primary teeth untreated include pain, infection (local and systemic) and abscesses. If parents have chosen not to seek early dental treatment for their child's carious teeth, extraction may remain as the only viable treatment modality. The reason for not seeking early dental treatment, is probably due to a lack of simple well-developed guidelines. Some form of guidelines to be followed by health workers would help greatly. Other reasons include inadequate knowledge regarding the importance of the primary dentition. The primary health care providers, who often see the child more frequently than their dental counterparts as well as parents are well placed to provide early care for children's primary teeth. Numerous studies have reported that dental caries is the principal cause of tooth loss in children,1-3 and that children with severe dental caries usually require extraction of several and, on occasions, all of their primary teeth. Part-I of this paper described the sequelae of dental caries. It is the purpose of this paper to highlight the consequences of providing only just the minimal treatment in the form of extraction of the carious teeth and to mention the other treatment options available if early treatment is sought. Effects of teeth extraction - Integrity and dimensions of the dental arch The primary dentition and the occlusal relationship of the maxillary (the upper teeth) to the mandibular (lower) teeth directly influence both the functional and morphological development of the permanent dentition.4 An important function of the primary teeth is to maintain the natural length of the dental arch and permit the permanent teeth to erupt in an orderly fashion with adequate space. Whilst it is uncertain that preservation of the primary dentition would prevent a malocclusion from developing in all cases, it has been shown that premature loss of primary teeth by extraction has a definite influence on molar occlusion and space in the permanent dentition.5-7 In regard to the frequency of occurrence of malocclusions, Willett8 stated that in 8% of cases, loss of primary teeth is the direct cause of a malocclusion; while in 52%, it is a supplementary cause. Furthermore, it increases the need for orthodontic treatment to correct the resultant crowding and malalignment of the teeth.5 A posterior cross-bite is one of the most common orthodontic problems and it is estimated that between 8% and 26% of children present with this type of malocclusion,9 which may be skeletal, or dental, or a combination of both in the primary dentition, and that this can lead to mandibular displacement accompanied by deviation of the lower midline.10 A vertical malocclusion, such as anterior open-bite, develops as a result of the interaction between many different aetiologic factors which include finger or pacifier sucking, lip and tongue habits, airway obstruction and true skeletal growth abnormalities.11 If extraction of a carious tooth occurs, the age of the child and the type of primary tooth that was extracted determines the extent of the subsequent space loss. Removal of a primary molar after the age of 7.5 years has minimal influence on space, whilst removal before this age leads to a loss of space which can sometimes be regained upon eruption of the permanent successor. Loss of a second molar before 7.5 years results in permanent loss of space due to the anterior drifting of the first permanent molar.5-7 Unilateral premature loss of a primary canine in a crowded dental arch can lead to a shift of the centre line which creates an asymmetric smile and is difficult to correct. Therefore, extraction of the primary predecessor disrupts the sequence and hence leads to a malocclusion in the permanent dentition. However, loss of a primary incisor after the eruption of the primary canines does not usually cause any space problem. The premature loss of a primary molar has been shown to affect the eruption time of the succeeding permanent tooth.12-14 For example, eruption of a premolar is delayed in a child who has lost a primary molar prematurely at 4 or 5 years of age. After the age of 5 years extraction of a primary molar gradually hastens the eruption of the premolar, such that, at ages 8, 9 and 10 years premolar eruption is greatly accelerated by the extraction of the primary molar.15 Under certain conditions premature loss of a primary molar will retard, or even prevent the eruption of the developing permanent successor,14 for which surgical removal of soft tissues and in some instances alveolar bone may even be necessary to encourage eruption. Speech It has been stated that speech development and the ability to articulate speech sounds are dependent on many related factors among which is the presence of the maxillary anterior teeth. These teeth serve as a landmark for the tongue and play a prominent role during the production of certain speech sounds.16 Of the six components necessary for the development of normal speech (respiration, phonation, resonation, articulation, neurologic integration and audition), articulation is the component most affected by the presence, or absence of teeth.17 The anterior teeth appear to be particularly important for the correct production of the /S/ and /Z/ sounds since their correct production necessitates forcing the air stream through an opening in the oral cavity which has to be small enough to produce friction noises.16 Therefore, the absence of incisor teeth is significantly related, in some children, to problems with the production of the /S/ and /Z/ sounds. However, such impairment is in most cases only transient as a growing child can overcome this problem with adaptive behaviour of the lips and the tongue.18 In addition, loss of maxillary incisors in children younger than 5 years of age is unlikely to result in defective articulation while the teeth are missing, or when the permanent dentition is acquired.19 Aberrant speech may be caused by factors other than loss of teeth, they are malocclusion, tongue tie, cleft palate, shortness of the soft palate; dentures or bridges planned without regard for phonetic consequences, and the fear of showing an unsightly diastema.20 The length of time that the teeth are missing is directly proportional to the type of the language problem produced.21 However, all children experience the effects of exfoliation of their primary teeth and chronic speech defects rarely result, so it is reasonable to assume that the premature loss of primary teeth seldom has any long lasting adverse influence on speech production in the majority of children. Mastication One of the obvious functions of the dentition is mastication of food. It is the first step in the digestive process and is under central control in the brain stem. The mechanical breakdown of foods makes enzymatic processing easier in the digestive system, and this mechanism is initially influenced by the way foods are chewed. It is a developmental function and its maturation occurs from learning experiences.22 If adequate, it provides the stimulus and proper function for the normal development of the maxilla and mandible. Generally, coordinated chewing is well established by 12 months of age; nevertheless, it continues to be refined during early childhood. Several factors potentially influence masticatory efficiency, including the severity of the malocclusion, occlusal contact area, body size, number of functional tooth units and the bite force.23 If a large number of primary teeth have to be extracted its worries parents about how their child will manage to eat. However, with the modern refined foods that Hong Kong children are eating, the need for mastication is negligible. So not surprisingly, the need to have teeth, in order to masticate effectively, has been doubted by some authorities who have even suggested that teeth are not essential!24 Appearance It is difficult to evaluate the significance of a pleasant looking set of teeth to a child. Different individuals have different attitudes towards their own teeth and their values are frequently influenced by prevailing social and cultural norms. In a society which places an increasing emphasis on aesthetics, it should be remembered that children also like to feel content about their appearance. They would like to have a set of teeth similar to those of their peers and thus avoid ridicule and criticism. Any criticism directed at a child's missing, or unsightly teeth may have a traumatic effect on his or her long term psychological development. Therefore, it can be seen that there is no valid reason for providing minimal treatment in the form of extraction which, in some cases, may be the only treatment option. However, a basic knowledge about the oral condition is necessary for the primary care providers who can offer first hand advice to parents and their children with whom they have a higher chance of having contact than their dental counterparts. In contrast, proper advice and referral made by them would give the parents a chance to seek for their children early dental care upon which, definitive yet specific treatment could be provided by dental practitioners to prevent future problems. Management of children with early childhood caries (ECC) Preventive measures Prevention should start in the pre-natal and peri-natal periods with nutrition and dietary advice to the mothers, especially during the third trimester of pregnancy, and for infants in the first year of life when the enamel on the teeth undergoes maturation.25 Expectant mothers should be educated about;
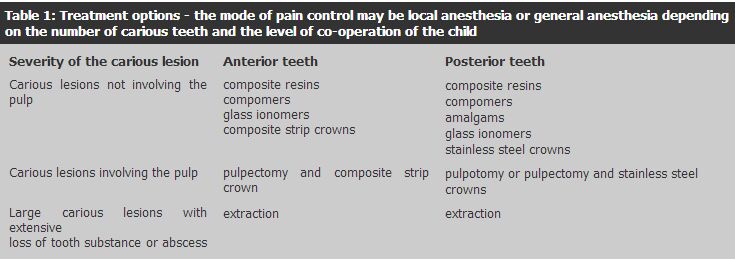
- the importance of nutrition throughout pregnancy Anxiety and fear Children are not small adults: their anatomy is different and they behave differently. Anxiety and fear can form a barrier and prevent the delivery of dental care as they lead to failed appointments, non-attendance and poor co-operation and disruptive behaviour in the dental environment. An understanding of these emotions helps the dentist to prevent, minimize or overcome these problems in the dental surgery. Pain control is thus an important aspect of dentistry for children. The available options are local anesthesia (LA), general anesthesia (GA) and inhalation sedation. Oral sedation can also be used but it can have less predictable outcomes which may compromise the treatment. Many children who have been labelled "uncooperative and unmanageable" can be treated successfully in the dental office under local anaesthesia with patience and suitable communication skills.26 Failing this, the child can be subjected to general anaesthesia to perform all of the treatment in a single session. Relative analgesia is only suitable for anxious children who are willing to cooperate. Restorative management Management of dental caries is multi-factorial. Prior to any definitive treatment plan the following factors must be considered;
- extent of the disease Restorative management of ECC is only the first phase of treatment and its success lies in maintaining a favourable oral environment. Therefore, treatment should be definitive yet specific for each individual child, with long term follow-ups and reinforcement of preventive measures. Restoration of primary anterior teeth (Figure 1)
The reason to restore carious primary incisors and canines is to allow the child to retain these teeth, so as to allow natural exfoliation without any pulpal complications. The options available are:
- restorations with composite resins, glass ionomer cements, compomers or stainless
steel crowns With bonded resin composite strip crowns it is possible to provide durable and aesthetically acceptable restoration of carious primary incisors.27 However, it is important to note that this is a technique sensitive procedure and requires good patient co-operation and optimal isolation. Nevertheless, these restorations have proven to be successful in terms of their esthetics and durability.28 Restoration of primary molars Depending on the extent of a carious lesion, the following materials can be used for the restoration of primary molars.
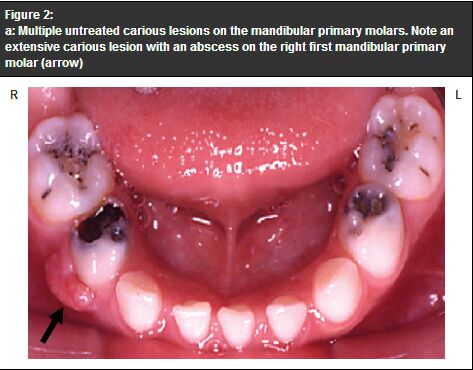
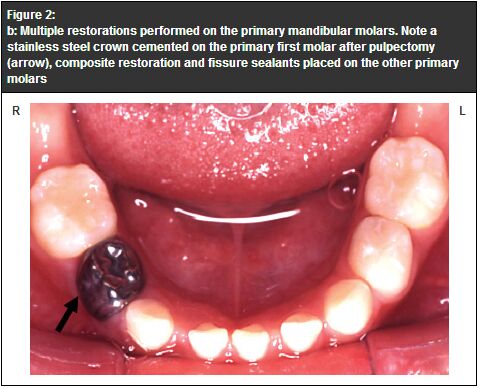
- amalgam Because of the controversies over the alleged health hazards of amalgam, it is becoming less commonly used. Hence, alternative materials like composites, compomers or GIC are more commonly used now and provide better aesthetics because they are tooth coloured. Pulpotomies are usually performed using Buckleys fromocresol in a 5 minutes application procedure to preserve the pulp tissue. When there is an extensive carious lesion in the molars (Figure 2a) the restoration of choice is a preformed metal crown (stainless steel crowns) see Figure 2b. A stainless steel crown covers the entire crown of the tooth so it decreases the number of tooth surfaces at risk from new caries. It is more robust and there is less chance of failure in comparison with all other restorative materials.29 However, the aesthetics are a compromise.
Fissure sealants They are recommended for primary and permanent molars in children with a history of dental caries and those who are in high risk groups. Fissure sealants have been proven to be effective; however, they need regular maintenance and repair.30 Prosthetic replacement / Space maintainers Premature loss of primary teeth by extraction has a definite influence on the occlusion and space for the teeth of the permanent dentition. Therefore, it is sometimes necessary to use suitable space maintaining appliances in an attempt to hold the space for the succeeding permanent teeth. Numerous factors such as age of the patient, teeth present, caries status, oral hygiene status, and willingness of the parents, and patient, for the treatments are among the factors that need to be considered prior to deciding to insert a space maintainer. Prosthetic replacements are rarely inserted, because the permanent teeth will erupt under the prosthesis which therefore necessitates frequent appointments. Furthermore, the presence of the prosthesis in the oral cavity can encourage plaque accumulation and caries in the abutment teeth. Prosthetic replacements cannot always be used because of behavioural issues that prevent the construction of the prosthesis and appropriate usage. Follow-up visits Frequent visits after restorative care lead to increased confidence and co-operation from the parents and the child because they involve preventive rather than invasive treatment. This also reduces the likelihood for the need of GA to retreat the child. This is important because it is unjustifiable to subject children to the risks and stresses of what is in principle an avoidable GA.31 Cost effectiveness of early dental visits Savage and coworkers,32 in their longitudinal cohort study among pre-school children, demonstrated a significant positive effect on dental related expenditures, with the average dentally related costs being less for children who received earlier preventive care. Children who have their first preventive dental visit before one year of age are more likely to have subsequent preventive visits, but not more likely to have subsequent restorative or emergency visits whilst, those who had their first preventive visit later are more likely to have subsequent preventive, restorative and emergency visits. The motivation of those parents who take their children for an early dental visit to provide the best possible oral health cannot be overlooked. Discussion It can been seen that there is no logical reason for leaving carious primary teeth untreated nor should the consequences of dental caries be treated solely by extraction of the affected teeth. While extractions may be the correct and necessary treatment option in some situations they should not be performed merely as the simplest solution, especially as the loss of the tooth may compromise the integrity of the dental arch. It should be remembered that the best space maintainer is a healthy or successfully restored tooth.33 It is essential that a parent finds a dentist who likes to work with children. Paediatric dentists are the paediatricians of dentistry and they are dedicated to meeting the unique dental needs of all children, including those with disabilities or special needs. Children are constantly growing and their treatment planning should be made by a specialist possessing a sound knowledge of the physiologic norms and variations in the developing dentition. Management strategies should encompass the most suitable options to arrest or minimize future complications. Intricate cases such as those children who have hypodontia (multiple missing teeth) or cleft lip and palate require a multi-disciplinary approach. The prevention of dental disease in infants and children begins with informed parents. A responsible parent, with the advice of a dental professional, is the one who must make decisions about seeking dental therapy. Enabling the parent to be an active participant in choosing preventive and restorative therapies can produce a better parent and induce child patient compliance.34 Sadly, in many cases, as a result of past experiences, parents assume that extractions are the only way to treat dental caries. Therefore, the dental professional is obliged to inform parents about, the need for specialist care, alternative therapies based on scientific evidence; risk assessments results, expected outcomes, possible complications and the cost. Conclusion Although dental caries remains the most common disease of the childhood, it can be prevented, provided it is identified at an early stage and the child is referred quickly, so that specific treatment based on the needs of the child can be delivered. In addition, basic knowledge about the importance of the primary dentition and the available restorative options allows the primary health care provider to deliver anticipatory advice to parents and children with whom they have an earlier contact than their dental counterparts. Key messages
Nigel M King, BDS, MSc (Hons), PhD, FDSRCS
Professor, Robert P Anthonappa, BDS, MDS (Paediatric Dentistry) Postgraduate Student in AdvDipPaediatrDent, Anut Itthagarun, DDS, PDipPaediatrDent, PhD Associate Professor, Paediatric Dentistry and Orthodontics, Faculty of Dentistry, The University of Hong Kong. Correspondence to : Professor Nigel M King, Paediatric Dentistry and Orthodontics, Faculty of Dentistry, The University of Hong Kong, Prince Philip Dental Hospital, Hong Kong.
References
|
|