
|
September 2005, Volume 27, No. 9
|
Original Articles
|
Outcome evaluation of ingrowing toenails managementSin-Ying Leung 梁善盈, Kwok-Man Lai 賴國民 HK Pract 2005;27:286-293 Summary
Objective: To evaluate the outcome of conservative treatment and
surgical intervention in the management of ingrowing toenails (IGTN) in Kowloon
East Cluster Podiatry in Hong Kong.
Keywords: Ingrowing toenail, nail surgery, nail care advice. 摘要
目的: 評估九龍東聯網足病診療服務以保守和手術治療趾甲內生的成效。
Introduction Ingrowing toenail (IGTN) is also called onychocryptosis. It occurs when the side of the toenail impinges into the nail sulcus skin with subsequent inflammation and sometimes infection.1 Hypergranulation maybe present (Figure 1). It is a common cause of pain in the big toe2 and it affects people of all ages. Clinical features include pain, local erythema and swelling of the toe. It affects gait, sports activities and increases difficulty in fitting footwear.3,4 The condition can be acute or chronic, with its course ranging from 1 day to years. Most IGTN occurs at the hallux.3 It is often related to poor nail cutting technique such as cutting too deep or leaving nail spike or shoulder at the nail corner. Ill-fitting footwear and trauma also contribute to the aetiology of IGTN.3 Podiatry receives referrals for management and advice for IGTN from various specialties, including Accident and Emergency Departments, Surgical Departments, Orthopaedics and Traumatology Departments, Skin Clinics, Family Medicine Clinics and General Out-patient Clinics (GOPC). GOPC accounts for the major source of referrals. The management of IGTN includes conservative treatment, e.g. nail wedge resection in clinical setting without local anaesthesia, nail care and footwear advice; and nail surgery under local anaesthesia. The commonest nail surgery is partial nail avulsion surgery with phenolisation of nail matrix. It is an effective surgery. This study was a prospective study on the outcome of IGTN management in the podiatry clinic in Tseung Kwan O Hospital. This involved the podiatry clinics of the Department of Integrated Rehabilitation Services in Tseung Kwan O Hospital and United Christian Hospital for conservative and surgical intervention for patients suffering from IGTN. 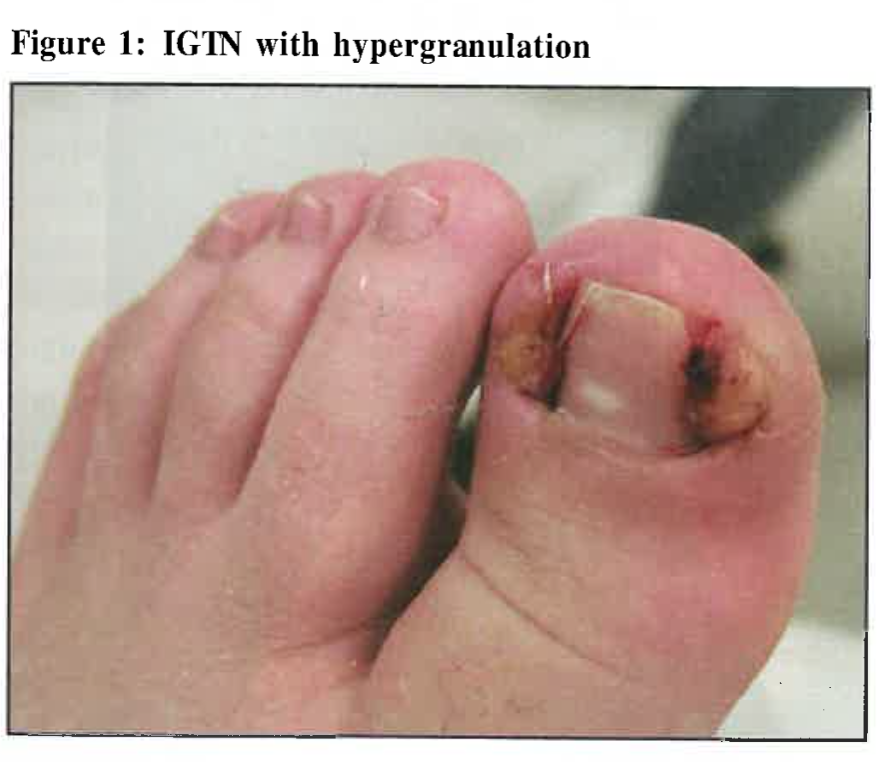
Literature review There are many options for treating ingrowing toenails. Conservative treatment is helpful for patients with a single episode of IGTN and can be successful with improved nail cutting technique and footwear. Advice for IGTN patients is listed in Figure 2 . If the condition recurs and conservative treatment fails, it is best treated surgically.5 For surgical options, there are a range of procedures including total or partial avulsion of toenail, matricectomy with carbon dioxide laser surgery, avulsion with excision of the germinal matrix, partial matricectomy followed by lateral fold advancement flap and partial nail avulsion with chemical cauterization of nail matrix using phenol or sodium hydroxide.1-2,6-13 Chemical matricectomy using phenol is one of the most common surgical procedures for permanent removal of problematic toenails.14 This procedure involves partial avulsion of the toenail and application of phenol to destroy the nail matrix. The nail will become narrower and application of phenol to the nail matrix can prevent the avulsed part of the toenail from growing back. Rounding and Hulm reviewed randomized controlled studies in the electronic database (CENTRAL, MEDLINE, EMBASE, CINAHL).1 It was concluded that phenolisation combined with simple avulsion of the nail was more effective than the use of more invasive excisional surgical procedures to prevent symptomatic recurrence at six months or more (OR 0.44 CI 95% 0.24 - 0.80). The addition of phenol, when performing a total or partial nail avulsion, dramatically reduced the rate of symptomatic recurrence (OR 0.07 95% CI 0.04 - 0.12). Fulton et al also found similar results and concluded that patients having wedge resection with phenolisation had a significantly lower chance of recurrence and better long-term results than a wedge resection alone in ingrowing toenail management.15 A randomized clinical trial by Gerritsma-Bleeker et al. found that partial matrix excision and phenolisation were equally effective in treating ingrowing toenails.3 To determine the outcome of the procedure, the rate of recurrence is the parameter of success. There have been many studies on the clinical outcome of nail surgery with phenolisation of nail matrix. In a retrospective study carried out by Andreassi et al to investigate the clinical outcome of phenol cauterization of the nail bed in treating ingrowing toenail during the period January 1996 to December 2001, it was found that the success rate was high with an overall recurrence rate of 4.3% (33 patients out of 764 patients) after 18 months.16 The success rates of other studies with smaller sample sizes were similar with recurrence of 0 to 4.4%.15,17 Number needed to treat was 1 to 1.05. There has been lack of research on the management of IGTN in Hong Kong. The aim of this study was to evaluate the outcome of conservative treatment and surgical intervention in the management of IGTN in Kowloon East Cluster Podiatry in Hong Kong. 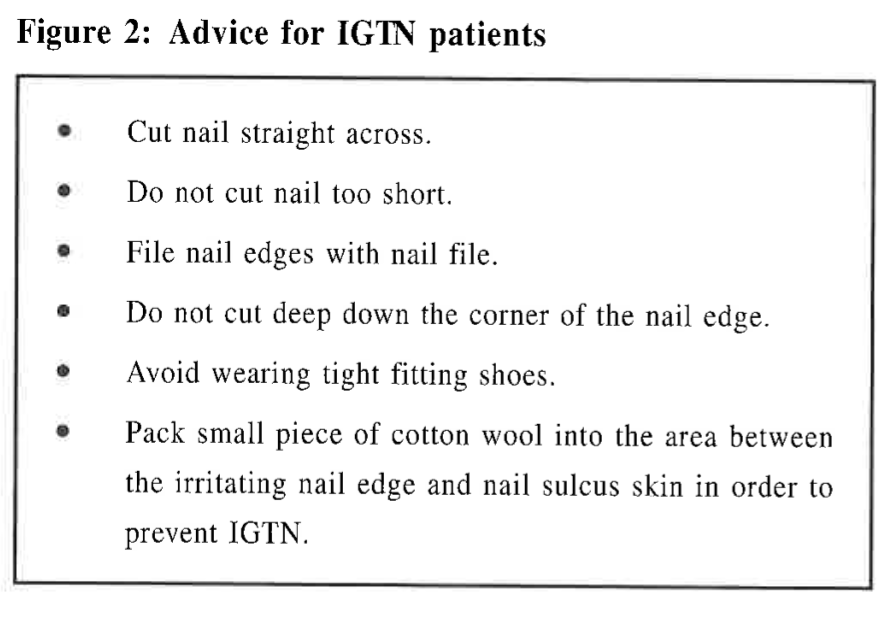
Methods This was a 2-stage prospective study. In Stage I, conservative treatment was used in treating IGTN and in Stage II, nail surgery was performed to treat recurrent IGTN. The flowchart in Figure 3 showed the design of the study. Convenient sampling was used to recruit subjects in Tseung Kwan O Hospital. New patients who presented with IGTN during the study period from March 2002 to February 2004, were invited to participate in the study. The purpose of the study was explained and verbal consent was obtained. Patients who were willing to participate in the study were known as subjects. 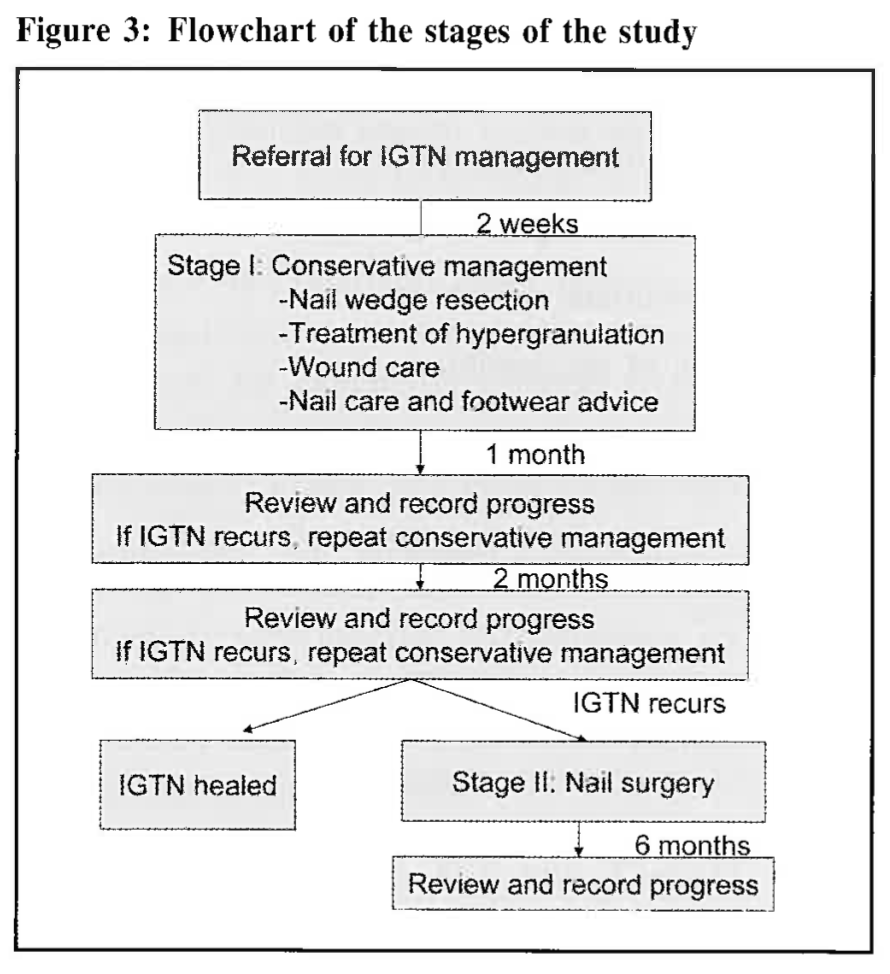
Inclusion criteria
- Clinically diagnosed big toe ingrowing toenail by medical officer Exclusion criteria
- Allergy to local anaesthesia Cases were seen in the podiatry clinic by referral. According to the triage system, IGTN cases were screened and seen within 2 weeks. The waiting time was kept to 2 weeks. A total of 178 patients suffering from big toe ingrowing toenail with one or both big toes affected were invited to participate in the study. The study was completed with 148 valid data. 30 subjects dropped out in Stage I mainly due to resolution of IGTN after the first or second consultation. They were counted as default cases. Default rate was 17%. Personal particulars, condition particulars and clinical outcome were recorded for analysis. Data collected included
1. Personal particulars e.g. sex, age Stage I : Conservative intervention In Stage I, the 148 subjects were treated conservatively in our clinic for the first 3 months. Procedures included diagonally cutting along the nail edge to remove the part of the toenail that was impinging into the nail sulcus skin (nail wedge resection) using podiatry instruments, treatment of hypergranulation tissue and wound care. Patients were referred to general out-patient clinic (GOPC) for daily dressing. To prevent recurrence, proper nail cutting technique, nail care and shoe advice were given. Nail care advice was listed in Table 1. In this stage, no invasive procedures were performed nor local anaesthesia was needed in the overall management. The patients were followed up after 1 and 3 months. The condition was re-assessed and recorded. Treatment would be performed if needed. Cases that did not respond to conservative treatment and presented with one or more recurrent episodes of IGTN at the end of three months post conservative treatment would be arranged for nail surgery (Stage II of the study) with consent. Stage II: Surgical intervention Thirty-four subjects with recurrent IGTN entered Stage II of the study. Nail surgery to these 34 subjects with 37 IGTN was arranged. Kowloon East Cluster podiatry team with podiatrists from Tseung Kwan O and United Christian Hospital performed the nail surgery to patients. Partial nail avulsion surgery with phenolisation of nail matrix was performed to the 37 affected toes under local anaesthesia (2% lignocaine plain). Subjects were reviewed regularly for wound evaluation until full recovery. During the healing period, patients were referred for daily GOPC dressing with special dressings provided by podiatry clinic. Their healing time and any recurrence were recorded. Result and outcome Subject profile Age
The age of the subjects (n=148) ranged from 1 year to 83 years (mean=38.41, SD+21.62). Sex
There were 77(52%) female and 71(48%) male subjects. Those who did not respond to
conservative treatment and entered Stage II for nail surgery were 10(29%) female
and 24 (71%) male. Number of IGTN episode and duration Ninety-eight (66%) out of the 148 subjects reported that it was their first episode of IGTN on the first date of consultation. 26% of the patients reported they had been suffering from the IGTN for less than 1 month, 30% for one to three months and 42% for more than three months. Source of referrals The majority of referrals were from GOPC (69%), AED (10%), Orthopaedics (7%) and Medical (7%).
The waiting time was 2 weeks. Table 1 shows the sources of the referrals of the subjects. 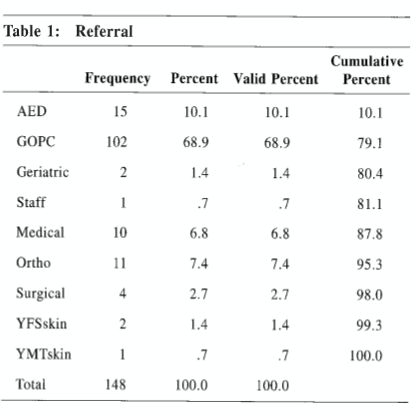
Outcome of Conservative Treatment Of the 148 subjects, 114 (77%) responded well with conservative treatment with no recurrence by the end of three months. Ten (7%) had recurrent IGTN in 1 month and a total of 34(23%) subjects had IGTN recurrence at the end of the third month. This recurrence group of subjects entered the Stage II of the study for nail surgery. Outcome of nail surgery Thirty-four subjects underwent nail surgery. Among these 34 cases, three subjects had bilateral toenail surgery. None of the subjects had recurrence of IGTN 6 months after the surgery. It was noted that the average healing time was 3.5 weeks. No wound complication was reported. All subjects reviewed 6 months after the surgery. After that, they were allowed to make follow-up appointments upon request within 6 months. Patients were subsequently discharged if they did not request a follow-up appointment. Discussion This study evaluated the outcome of the conservative management and nail surgery for IGTN. The results showed that conservative treatment was helpful for immediate pain relief and had high success rate (77%). Number needed to treat was 1.4. Success in treatment was found to be related to age and sex. Female and relatively older patients were found to respond better to conservative treatment. Since it is important for patients to perform proper nail care and improve footwear to prevent recurrence in conservative treatment, this group of patients might be more willing in learning nail cutting technique and changing into better footwear. As conservative treatment is non-invasive, cost-effective and can be readily performed in out-patient settings, it should be the primary treatment for all IGTN patients before considering surgical options. Nail surgery has high success rate and is a good treatment option for long term management of IGTN. In this study, the rcurrence rate in 6 months was 0% (n=34). This rate was comparable to recurrence rates in other studies.3,15,17 The toenail became narrower after surgery and the irritating part of the toenail would not grow back. Figure 4 shows a picture of a healed IGTN post nail surgery. In the daily practice of podiatry, conservative treatment is the first choice of management as it is quick, cost-effective, produces minimal pain or bleeding and gives patient immediate relief. The wound caused by the nail impingement usually heals within two days to one week after nail wedge resection. Patients will not face the risks of nail surgery complications such as post-op wound pain or bleeding. The time needed to perform conservative treatment is only 10 to 20 minutes including nail wedge resection, treatment of hypergranulation tissue and advice on proper nail cutting technique and footwear. The appointment waiting time is 2 weeks. Nail care advice compliance is the key of success and it can reduce chance of future recurrence of IGTN. If the condition does not improve with conservative treatment, surgery should be arranged for long term management. Nail surgery with the use of phenol to nail matrix is very effective. The average waiting time for surgery is 2 weeks for urgent cases to 12 weeks for regular cases. Although the post-op wound takes longer to heal (3.5 weeks) and the nail will be permanently narrower than before operation, it gives excellent outcome and patient satisfaction. 
Recommendation IGTN is a common foot disorder for any age. The first healthcare practitioner that patients consult are family physicians. Conservative management including nail wedge resection and nail care advice can be performed in the out-patient setting. Good technique for nail wedge resection and comprehensive nail care advice can prevent future recurrence of IGTN. For recurrent or complicated cases, such as patients with diabetes or ischaemia, early referrals to podiatry can be made for management. Patient will benefit from holistic care from nail care and footwear advice, conservative intervention, nail surgery to post-op care in podiatry clinic. Post surgery care is important to prevent infection and promote healing. This involves cooperation with GOPC for patients' daily wound dressing. Good communication would be important between podiatrists and GOPC colleagues in the management of IGTN. Workshop can be held for inter-discipline sharing of IGTN management to improve skills and reduce patients' suffering. Further studies can be carried out with larger sample size and comparison with other populations. Conclusion Both conservative and surgical management for IGTN were effective and gave good outcome and patient satisfaction. Conservative treatment should be the first line of management as it is less time-consuming, more cost-effective and has less complications than surgery. It can also be readily performed in an out-patient setting. Surgery is very effective but has longer waiting time and is more time-consuming. It can be the second line of management when patients do not improve with conservative management. Podiatry referrals can be made for recurrent or complicated cases. More communication between podiatrists and clinical staff of GOPC, such as workshop sharing, should be promoted so that more patients can benefit. Further study with larger sample size and comparison of other populations is suggested. Key messages
Sin-Ying Leung, BSc(UK), MSc(CUHK)
Podiatrist, Department of Integrated Rehabilitation Services, Tseung Kwan O Hospital. Kwok-Man Lai, DPodM Podiatrist, Podiatry Department, United Christian Hospital. Correspondence to : Miss Sin-Ying Leung, Department of Integrated Rehabilitation Services, Tseung Kwan O Hospital, 2 Po Ning Lane, Hang Hau, Hong Kong.
References
|
|