|
February 2003, Volume 25, No. 2
|
Original Articles
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
What do family medicine trainees say about their training?Y T Wun 溫煜讚, T P Lam 林大邦, L C Y Tsang 曾昭義 HK Pract 2003;25:59-69 Summary
Objective: To survey the vocational trainees' evaluation of their
training.
Keywords: vocational training, family medicine, evaluation study, Hong Kong 摘要
目的: 調查家庭醫學學員對他們所受職業訓練評價。
Introduction The Hong Kong College of Family Physicians (HKCFP) has been organising vocational training for family medicine since 1985. In 1998 there was a surge in the number of trainees when the Hospital Authority introduced family medicine trainee posts for junior doctors. The training programme consists of two-year rotations in different hospital specialties (Basic Hospital Training), two-year community-based outpatient clinics (Basic Community Training), and then two-year Higher Training in community-based clinics (Higher Training). The trainees are assessed by examination after the basic training, leading to Fellowships in HKCFP and Royal Australian College of General Practitioners (RACGP). Successful trainees enter Higher Training, at the end of which they undertake the Exit Examination leading to the Fellowship of Hong Kong Academy of Medicine. Although the trainees are assessed by examinations, their evaluation of the training programme has never been analysed. Some countries have evaluated their vocational training programmes after running for some years.1,2 An essential step in such evaluation is getting feedback from trainees.3 In May 2002, we conducted a questionnaire survey of all the trainees, present and past, for views on their training. Our aim was to collect their opinions and experience about their training, especially around the time when the first batch of trainees from the Hospital Authority were about to finish their four-year Basic Training. We hope that the results will provide impetus for further improvement of the training programme. Objective To identify factors which Hong Kong primary care doctors perceived as salient in establishing or sustaining doctor-patient relationships. Method We designed a questionnaire comprising three parts:
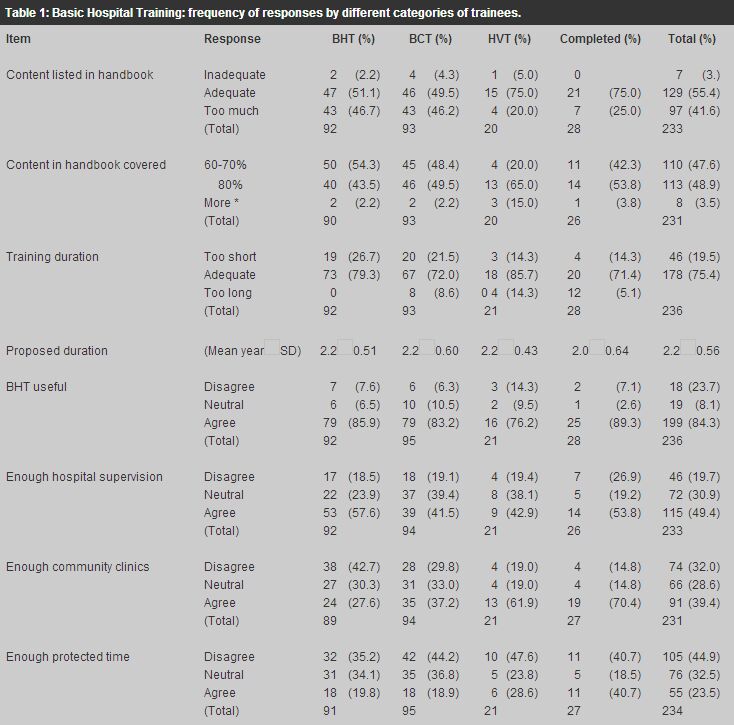
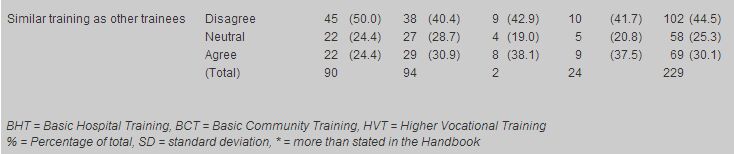
With the permission from the Board of Vocational Training and Standards, we obtained a list of trainees registered with HKCFP. To encourage response, the questionnaire was anonymous. The return-envelops were numbered and only the research assistant knew the number of each trainee on the master list. Due to the small numbers of "strongly disagree" and "strongly agree" answers, we present our results after combining "strongly disagree" with "disagree" into "disagree", and "strongly agree" with "agree" into "agree". For the qualitative section, the open responses were recorded verbatim into a computer file. For ease of reference in reporting the results, the research assistant randomly numbered each returned questionnaire. We read through the printouts independently and discussed the themes to be extracted. WYT then did the thematic analysis and circulated the results to the other authors for discussion. Chi-squared test was used for quantitative analysis, with p=0.05 as type I error. Results The questionnaire was sent with an explanatory letter to 360 past and present trainees. One replied that he/she was not a trainee. Three were not trained in Hong Kong, and one could not be contacted due to the wrong address. There were 32 higher trainees, 162 hospital-based trainees, 101 community trainees, and 2 deferred training, making a total of 297 current trainees and 58 past trainees. After three rounds of invitation, 247 returned the questionnaires, a response rate of 70% (247/355). Response rates from hospital-based trainees were 92/162=56.8%, community-based trainees 93/101=92.1%, higher trainees 20/32=62.5%, and those who had completed training 28/58=48.3%. Basic hospital training Table 1 shows the responses from the trainees grouped by their current stage of training. Overall, 84% trainees found hospital training useful, and 75% thought two-year training was adequate. As to the content listed in the handbook, 41% considered it too much and 48% had covered only 60-70%. Only 49% trainees agreed that they had adequate supervision, 39% had adequate training in community-based clinics, 24% had adequate protected time, and 30% had been treated equally as other specialty-trainees.
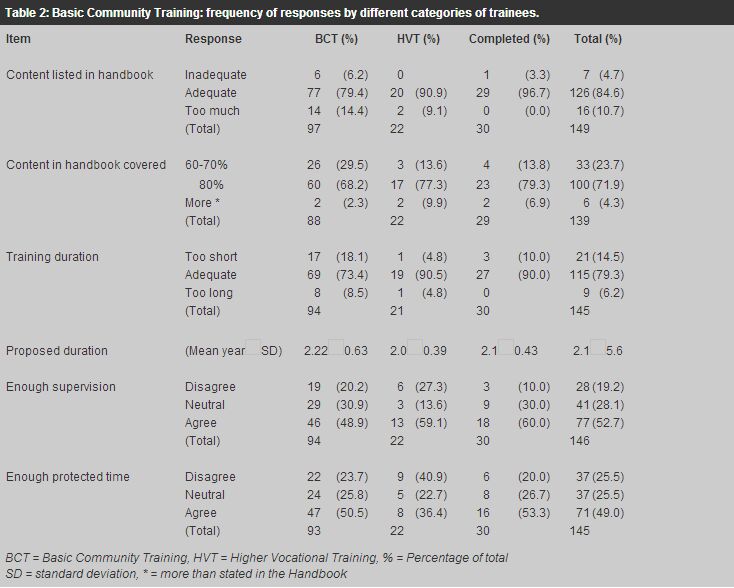
Basic community training Although 85% of all the trainees considered the content in the handbook adequate, 24% could cover only 60-70% (Table 2). Most considered two years to be adequate for the training. Only 50% of the trainees agreed that they had adequate supervision or protected time. (A quarter of trainees in basic training (hospital and community combined) regarded two-year to be too short but only 14% of the higher and past trainees thought so. The difference was not statistically significant (c2=2.05, p=0.36)).
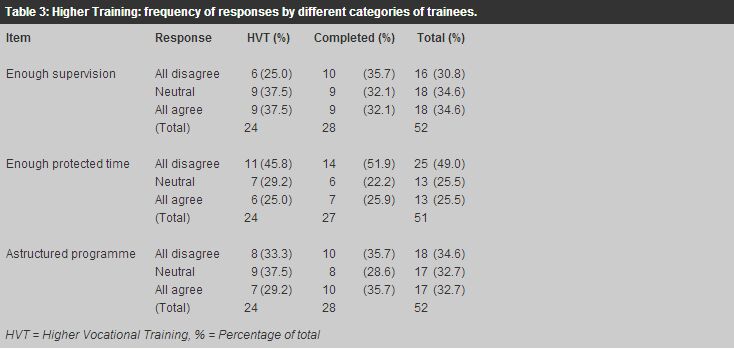
Higher vocational training Only half of the trainees agreed that they had adequate protected time (Table 3). Regarding supervision and the structure of the training programme, they were equally divided into "agree", "neutral", and "disagree".
What supervision do they have? Comments on the Basic Hospital Training unanimously voiced frustration. They felt neglected, their role misunderstood, and inadequately supervised.
Comments on the Basic Community Training are about equally positive and negative. It seemed that the quantity as well as quality of supervision varied. Some positive comments included:
But there were also negative and contradictory comments.
Similarly, the comments on supervision in Higher Training are conflicting, e.g.,
How did their colleagues treat them? Comments from the Basic Hospital Trainees were unanimously bitter. They were the only category of trainees giving comments to this theme. Marked frustration was shown, e.g.,
What have they learnt? Trainees in Basic Hospital Training expected also some training in family medicine but were generally disappointed.
Basic Community Trainees often found their expectation met, apparently with some hard effort.
Having gone through with basic training, Higher Trainees generally found themselves not learning many new things. They also felt isolated.
Comments on seminars All the trainees have seminars; some had protected time for them but more did not. The trainees themselves ran these seminars and the comments were unfavourable. The Basic Hospital Trainees had negative comments on the seminars.
But the other trainees were also dissatisfied with the seminars. The Basic Community Trainees commented:
The same comment from the Higher Trainees:
How useful is the training? Despite much dissatisfaction and uncertainties, the overall comment of the training by the trainees was positive. Most thought that they had gained knowledge and skill. The comment "satisfactory" came from far more trainees than "disappointed".
Dissatisfaction with the training came less from the content than the uncertainty of the future and self-esteem, especially for the basic trainees under contract. "No future", "Nowadays, in Hong Kong health policy, no one will really help the junior doctor for training/career" and "Have I made the wrong decision for choosing family medicine in my career" were examples of despair. These are also reflected by comments like:
Constructive suggestions Many trainees did not just tell their problems but also suggested solutions. They did not complain about the HKCFP, but suggested that the College should proactively promote communication between the College and the hospital specialists, the supervisors and the trainees. The College should have the obligation to monitor the quality of training. For example,
Discussion This study shows that the trainees are satisfied with the nature of their vocational training but not the process. Most grievances relate to the Basic Hospital Training. Their grievance may be due to misunderstanding the purpose of training family medicine in hospitals. The ward staff may have difficulty in adjusting to a trainee who will not stay long. The seniors who are mostly service-oriented are inexperienced in dealing with these trainees for short periods. Similar feelings were observed in the United Kingdom: "Education and training in hospital-based vocational training posts was widely perceived as being of poor quality, of little relevance to general practice careers and treated as being of secondary importance to meeting service commitments".4 The Basic Community trainees are satisfied with their training, probably because they are more accustomed to doing family medicine. Their comments are diverse but balanced. The important comment is on the supervisors. There are two problems: inadequate trainers and lack of quality control. Some trainers are obviously dedicated and capable, earning high appreciation from the trainees, while some may not understand their role. The expectations of trainers and trainees should be explicit and congruent. Most Higher Trainees comment on the lack of a structured programme. While a structured programme is mandatory for Basic Training, it may not be so for Higher Training. With the FHKCFP and FRACGP qualifications, the Higher Trainees should be able to practice independent quality FM. But if the Higher Trainees cannot improve their knowledge and skill during their training, the objectives of Higher Training have to be reviewed. "The higher training should enable our trainees to process special skills on special interests rather than repetition of basic training and make up a programme". (#55) Audit, practice management, and consultation skills are not just "exam papers" but advanced skills for them to learn. These are also important life-long skills for continuous professional development. "More practical guidelines/information needed from experienced general practitioners as those information are difficult to obtain from textbooks" (#1) is very true. The findings of this study repeat what have been observed a decade ago in the United Kingdom, Ireland, and New Zealand: lack of protected time for teaching, absence of structured programme, and no clear indication of what to teach in hospital rotations.3-7 It is specifically pointed out that "The concept of protected time for teaching, which is a feature of the general practice component of training, is not one that is readily accepted by many hospital consultants", and that "An important difficulty is that of balancing the time needed to fulfill the service commitments of all hospital posts with the time needed for learning and teaching". We are surprised by the good response from the trainees and the voluminous comments and suggestions written; some of which are so frank and opened. We cannot agree more that "Feedback from trainees very important" (#28). To evaluate training, the trainees should not only be assessed but should also have the opportunity to assess. Given the variable quality of seminars, supervisors and trainers as opined by the responding trainees, the College should have quality assurance on its vocational training: training programme, trainers and trainees. "Trainee does not know what they should learn. Trainer did not know what they should teach in the past but also prepare to change in the future". (#9) We conclude that there is the urgent need for improved communication between the trainees and the College (to clarify the objectives of training and discuss the feedback on training itself), between the College and the supervisors (to clarify the supervisors' role and ensure quality of supervision), and between the trainees and the supervisors (to make training more fruitful). There are of course limitations on what we can do, e.g., employment opportunities for trainees. Although employment opportunity could affect immensely the motivation and perceived satisfaction of vocational training, we should evaluate training by the knowledge, skill and attitude in family medicine ultimately achieved. Training and learning can be a painful process with falls and hurt. Success is not given but achieved with continuous evaluation and effort. We hope that this study can suggest directions for improvement and facilitate the relevant organisations in enhancing vocational training to be a greatly treasured experience. Acknowledgement We thank all the trainees who responded to our questionnaire, especially those who expressed their views and feelings. We thank them not just for their response, but also for their openness in expressing their opinions and the trust they gave us for ensuring anonymity and confidentiality. Our special thanks are to Mr. Peter Chan, research assistant of Department of Community and Family Medicine, The Chinese University of Hong Kong, for his hard work in data processing and analysis. Key messages
Y T Wun, MBBS, MPhil, MD, FHKAM(Fam Med)
Member,Research Committee, The Hong Kong College of Family Physicians,Formerly, Department of Community and Family Medicine, The Chinese University of Hong Kong. T P Lam, MBBS(W Aust), MFM(Monash), PhD(Medicine, Sydney), FRACGP Associate Professor, Family Medicine Unit, Department of Medicine, The University of Hong Kong. L C Y Tsang, MBBS, DFM(CUHK), FRACGP, FHKAM(Fam Med) Consultant Family Physician, Training Centre in Family Medicine, Department of Health, Hong Kong SAR. Correspondence to : Dr Y T Wun, Research Committee, HKCFP, Room 701, HKAM Jockey Club Building, 99 Wong Chuk Hang Road, Aberdeen, Hong Kong.
References
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||