|
October 2002, Volume 24, No. 10
|
Original Article
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
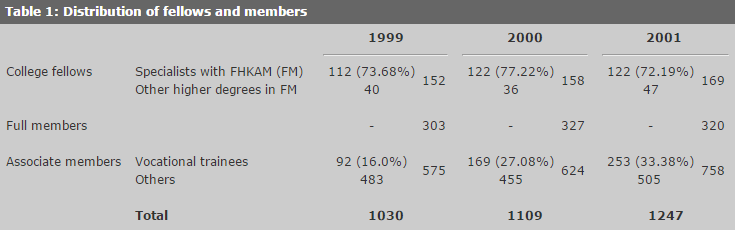
A review of the impact of CPD on QA activities: a study from 1999-2001K W Chan 陳國維 HK Pract 2002;24:474-479 Summary Objective: Since Continuous Professional Development (CPD) was introduced into the Hong Kong College of Family Physicians' Quality Assurance (QA) programme in the 2000, there has been concern that CPD activities were tedious, time-consuming and difficult to achieve. This paper analyses the impact of the additional CPD component on the award of QA certificates. Design: Retrospective study. Subjects: All records of educational activities of members and fellows of the Hong Kong College of Family Physicians from 1999 to 2001 were extracted from the College computer for analysis. Results: In the first year after the introduction of CPD, there was initially a significant drop in the award of QA certificates among College Fellows (from 90.13% to 78.48%) and Full Members (from 35.64% to 28.13%). This returned to normal in the following year. The learning patterns of our members after the introduction of CPD were also analysed. Although CME activities were still the most common learning tools, CPD activities had been utilised well above the QA certificate's minimal requirement of 5 CPD credit points per year. The mean annual CPD scores of College Fellows and Full Members were around 19 credit points and that of Associate Members were 14 credit points. Keywords: CPD, CME, quality assurance, learning behaviour 摘要 目的: 香港家庭醫學學院的質素保證計劃在 2000年開始引入持續專業發展概念(CPD)後,其會員多關注到 CPD 活動的沉悶、費時,以及不易取得 CPD 學分。本文分析附加的 CPD 部份對進修証書頒發所造成的影響。 設計: 回顧性研究。 對象: 從香港家庭醫學學院的電腦資料,分析包括 1999至2000年內所有會員和院士的學習記錄。 結果: 在引入 CPD 後的首年,香港家庭醫學學院院士和正式會員在取得進修証書方面,初期顯著減少,分別由 90.13% 降至 78.48% 及由 35.64% 降至 28.13%。自質素保證委員會推廣後,跌幅在其後一年回復正常。本院會員的學習模式亦加以分析。延續進修仍是本院會員最常採用的學習工具,但是 CPD 活動遠遠超過進修証書規定每年5個 CPD 學分的最低要求。學院院士和正式會員每年的平均 CPD 學分是19分,而副會員是14分。 主要詞彙: 持續專業發展概念,延續學習進修概念,質素保證,學習行為 Background The medical profession is confronted with increasing demands in order to ensure and to improve the care of patients. As a result, Continuous Professional Development (CPD)1 was first introduced in the United Kingdom in 19982 as a means to link medical education with the quality of care. While CPD is gradually accepted by the medical profession for Quality Assurance (QA), the speed of moving from the traditional CME based QA programme to those CPD based QA programmes should be gradual and accepted by the profession.3 The Quality Assurance and Accreditation (QA&A) committee of the Hong Kong College of Family Physicians started to incorporate CPD activities into the QA programme in 2000 in order to promote self-directed active learning. The main CPD activities include clinical audits, learning plans in the form of CPD logs, supervised clinical attachments organised by the College and small learning groups with assessments and reviews. Cardiopulmonary resuscitation (CPR) courses and those activities that require interactive teaching of family medicine and post-course professional examinations/assessments are also included. To be awarded the QA certificate, College members must obtain, within a one year period a total of 30 credit points, 5 of which must be from CPD activities. There are 7 types of membership in our College: College Fellows, Full Members, Associate Members, Affiliate Members, Student Members, Non-HKSAR Fellows and Non-HKSAR Members.4 Both College Fellows and Full Members are practitioners predominantly engaged in family medicine for not less than five years. College Fellows, in addition, must possess a higher degree in Family Medicine. Over 70% of our College Fellows also possess the specialist degree FHKAM(Fam Med) and are specialists in Family Medicine (Table 1). There is a legislative requirement that all specialists need QA certificates to maintain their specialist status. A family medicine specialist who fails to maintain the QA certificate for 3 consecutive years shall be suspended.5 Introduction Since the introduction of the CPD component into the QA programme, there has been concern that CPD activities were tedious, time-consuming and difficult to achieve. This paper analyses the impact of the additional CPD component on the award of QA certificates to the different categories of members. It also reviews the learning behaviour of our members after the introduction of the CPD activities. Method All College Fellows, Full Members and Associate Members of the Hong Kong College of Family Physicians in Hong Kong are automatically registered with the College's Quality Assurance (QA) Programme. While their registration with the College's QA Programme is automatic, their participations in educational activities are voluntary and therefore are suitable for analysis. All records of their educational activities from 1999 to 2001 were analysed. 2 (row) x 3 (column) Chi-square tests were used to analyse the awards of the QA certificates within the 3 years study period (Table 2). The percentage of members awarded QA certificates was calculated by dividing the number awarded by the total of number of members in that category as listed in the College registry. As CPD was introduced into the QA programme in 2000, 1999 was the pre-CPD year and its records were used as a baseline reference. 2 2 Chi-square tests were used to compare the awards of the QA certificate in the CPD years 2000 and 2001 against those in year 1999 (Tables 3 and 4). Records of the educational activities in 2001 were further analysed to reflect the learning pattern of different categories of members after the introduction of CPD (Table 5). Results Over 1000 College Fellows or Members were included in this study. The distribution of their categories of membership was shown in Table 1. The ratio of College Fellows to Full Members and to Associate Members was around 1:2:4 (150:300:600).
The awards of QA certificates were tabulated in Table 2. In 1999, 137 (90.13%) College Fellows, 108 (35.64%) Full Members and 70 (12.17%) Associate Members were awarded QA certificates. A Chi-square value of 349.22 with 2 degrees of freedom rejected the null hypothesis and affirmed that College Fellows, Full Members and Associate Members differed in their awards of QA certificates. Similar results were also observed in year 2000 and year 2001.
The awards of QA certificates between the CPD and pre-CPD years were compared in Tables 3 and 4. After the introduction of CPD in 2000, there were significant drops in the QA certificate awards among College Fellows (from 90.13% to 78.48%) and Full Members (from 35.64% to 28.13%) (Table 3). The Associate members, however, were not affected. In the following year 2001, this falling trend was reversed and there was no significant different drop in the QA certificate awards among the College Fellows and Full Members. The awards of QA certificate to Associate Members had increased significantly from 12.17% in year 1999 to 17.81% in year 2001.
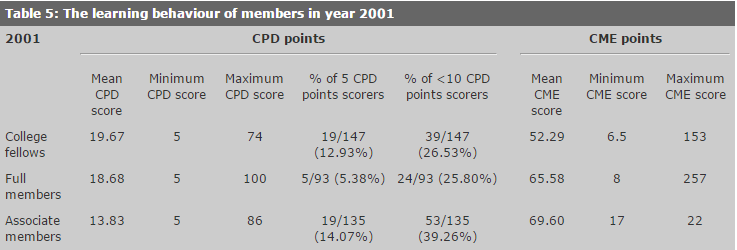
The learning behaviour of our College Fellows and Members in 2001 was analysed in Table 5. CME was used extensively among College Fellows, Full Members and Associate Members as a learning tool. The mean CME scores in all 3 categories were over 50. The mean CPD scores were lower and ranged from 13.83 credit points among Associate Members, to 18.68 credit points among Full Members and to 19.67 credit points among College Fellows. All these figures were well above the minimum requirement of 5 CPD points for the award of the QA certificates. However, there was still around 5 to 15% of our College Fellows and Members who gained just the bare minimum 5 CPD points for their QA certificate.
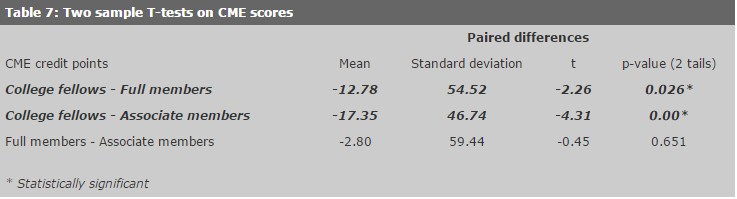
Statistical analysis using 2 sample T-tests showed that both College Fellows and Full Members had significantly higher CPD scores than Associate Members (Table 6). On the other hand, Associate Members and Full Members had significantly higher CME scores than College Fellows (Table 7).
Discussion Around 80% of College Fellows were awarded QA certificates. Most of them were specialists in Family Medicine, who by law, need the QA certificates to maintain their specialist registration. This figure of 80% was significantly higher than the 30% of Full Members and the 15% of Associate Members as these latter 2 categories of members did not have any legislative requirement on compulsory QA activities. Similar figures and patterns were observed throughout the 3 years' study period, irrespective of whether CPD was included in the QA award requirements or not. All specialists in Family Medicine had their QA certificates awarded throughout the 3 years under study. If we exclude these Family Medicine Specialists from the College Fellows and look at the figures again (Table 8), we found that the percentage of awards of QA certificates dropped to around 60% except in year 2000 when CPD was first introduced. This demonstrated the trend in awarding the QA certificates: 100% among Family Medicine Specialists, 60% among College Fellows, 30% among the Full Members and 15% among Associate Members.
As specialists in Family Medicine received more training than College Fellows who in turn received more training than Full Members, one may conclude that training can improve the number of doctors undertaking QA educational activities. Legislation, however, is the most powerful motivator, as 100% of the Family Medicine Specialists obtained their QA certificates. The impact after the introduction of the CPD on the awards of the QA certificates were analysed in Tables 3 and 4. There were significant drops in the percentages of College Fellows and Full Members being awarded QA certificates in 2000, when compared with the pre-CPD year of 1999 (Table 3). Reasons include extra time, extra workload and the unfamiliar new CPD concept. To help members to overcome these barriers, the QA&A committee organised workshops to promote the concept of CPD and to emphasise the gains in performing CPD, namely, improving quality of care, gaining skills that meet the learner's needs yet at a pace determined by the learner and saving the time cost of being physically present at venues or at boring lectures etc. Articles on Quality Assurance6 and CPD1 were published in the College Journal, the Hong Kong Practitioner. After a series of such campaigns, the QA certificates awarded to percentages of College Fellows and Full Members rose in 2001 back to a level that were not statistically different from their corresponding pre-CPD percentages in 1999 (Table 4). The impact of CPD on Associate Members was somewhat different. There was no significant difference in the percentages of the award of QA certificates between the year 2000 (14.26%) and that of the pre-CPD year 1999 (12.17%). One reason being that the actual percentage of Associate Members who obtained the QA certificates was low (only 10% to 15%). Also, among those who obtained the QA certificates, a significant proportion were from vocational trainees. The impact of CPD on vocational trainees was not as great as on others as trainees received supervision from their mentors and supervisors. This, together with the substantial increase in the number of trainees from 92 in year 1999 to 253 in year 2001 (Table 1), explained why the percentage of QA certificate awarded could rise even further in 2001 to 17.81%, a figure which was significantly higher than the pre-CPD year 1999. Conclusion QA certificates are awarded to College Fellows, Full Members and Associate Members after they have satisfied the requirements on Quality Assurance. The difference in award of the QA certificates among the different categories of membership demonstrated that without regulations and enforcement, the participation in QA programmes would be low. The 1999 figures: 100% among Family Medicine specialists as compared to the 62.55% of non-specialist College Fellows, 35.64% of Full Members and the 12.17% of Associate Members were illustrative. CPD was first introduced into the College's QA programme in 2000 as a means to promote self-directed learning. This had resulted in a significant drop in the percentage of College Fellows and College Full Members who obtained QA certificates in that year. The figures rose back in 2001 to the pre-CPD level after a series of campaigns from the QA&A committee. Changes made to the QA programmes could have been a burden to members, resulting in the initial drop. If these changes were to be successfully implemented, there should be adequate support and backup for members. The learning patterns of our members after the introduction of CPD were analysed. Although CME activities were still the most commonly used learning tools, CPD activities had been utilised to an extent well above the QA's minimal requirement of 5 CPD credit points per year. The mean annual CPD scores of College Fellows and Full Members in 2001 were around 19 credit points and that of Associate Members was 14 credit points. Although College Fellows and Full Members used more CPD activities than Associate Members, around 25% of them still had CPD scores below 10 credit points. More effort from the QA&A committee are needed to help these 25% of members since in 2002 the College has increased the CPD requirements for the award of the QA certificate from 5 to 10 CPD credit points a year.
K W Chan, MBBS, FHKAM(Family Medicine), FRCGP, FRACGP
Chairman, QA&A Committee, HKCFP. Correspondence to: Dr K W Chan, , The Hong Kong College of Family Physicians, 7th Floor, HKAM Jockey Club Building, 99 Wong Chuk Hang Road, Hong Kong. References
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||