|
September 2015, Volume 37, No. 3
|
Update Article
|
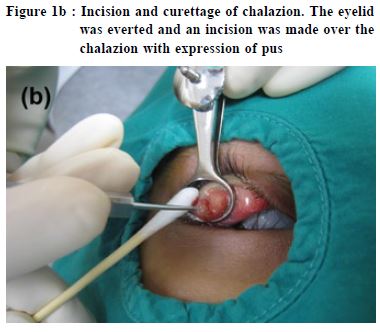
Common eye infections: causes, clinical features and managementShiu-ting Mak 麥兆婷 HK Pract 2015;37:93-100 Summary Eye infections can affect one or both eyes, and occur at any age. While some eye infections are mild and may even resolve without treatment, severe infections may result in permanent visual loss if not treated in a timely manner. Primary care physicians are often the first line of contact for patients presenting with eye infections. Thi s a r t icle a ims to r ev iew the causes , cl inica l features and management of eye infections commonly encountered in primary care practice. 摘要 眼部感染會影響一隻或兩隻眼睛,並可在任何年紀發 生。一些輕微感染,或可不藥而癒。但嚴重的,若未能 及時醫治,卻會引致永久性視力障礙。基層醫療醫生往 往是眼部感染病人最早接觸的醫療人員。本文旨在評述 基層醫療中常見眼部感染的成因、臨床徵狀和療法。 lntroduction Eye infections are commonly bacterial or viral in nature. They may occasionally also be caused by fungi and rarely by parasites. Infections can involve the eye and/or the tissue immediately surrounding the eye, including eyelids and the lacrimal passages. Eye infections can affect one or both eyes, and may occur at any age. This article reviews the causes, clinical features and management of eye infections commonly encountered in primary care practice. Eyelid infections Hordeolum and chalazion Hordeolum is a common, painful inflammation of the eyelid margin that is usually caused by bacterial infection.1 It may involve meibomian glands of the eyelids resulting in internal hordeolum, or hair follicles of the eyelashes resulting in external hordeolum, also known as stye. It commonly occurs following blockage of oil glands with secondary bacterial infection, most often Staphylococcus aureus. Patients with hordeolum often present with a red, painful eyelid swelling. It has been suggested that size of the swelling is a direct indicator of the severity of infection.2 The infection may spread to neighbouring ocular tissues and result in preseptal cellulitis. Recurrence is common, and is usually the result of failure to eliminate the existing bacteria completely rather than caused by new infections.3 Persistent styes may lead to chronic inflammation resulting in formation of chalazion (Figure 1a). Hordeolum often resolves on their own. Initial treatment is mainly conservative, involving application of warm compresses several times a day. Better eyelid hygiene is beneficial. Patients should be taught to dip a clean cleansing cotton into warm, boiled water, swiping it from the inner corner to the outer corner of the eye, gently scrubbing the eyelids especially the root of the eyelashes along the way. The cotton should be swiped along a single direction once only and must not be reused. A topical antibiotic may be prescribed in conjunction to prevent spread of infection. The natural history of acute hordeolum generally spans one to two weeks.1 If the condition is severe or resistant to conservative management, systemic antibiotics or surgical incision and drainage may be required (Figure 1b). 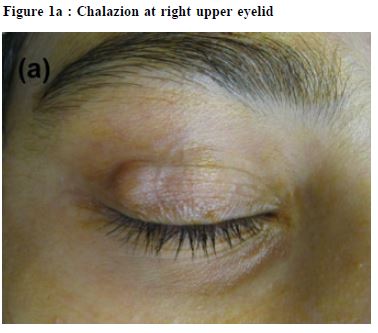
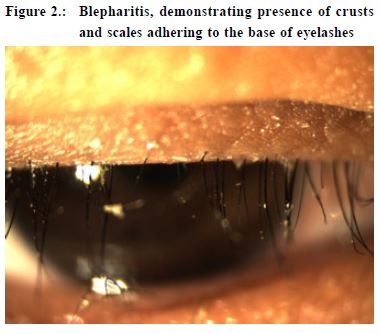
Blepharitis Blepharitis, defined as inflammation of the eyelids, may be acute or chronic. Acute blepharitis is referred to as lid infection by some, and may be bacterial, viral, or parasitic in etiology.4 It is commonly a result of Staphylococcal infection. The glands near the eyelid exhibit excessive oil production and create a favourable environment for bacterial growth. Patients with blepharitis usually present with red eyelids, itchiness and irritation. Sometimes, crusts and scales may be found adhering to the base of the eyelashes (Figure 2). Staphylococcal blepharitis is characterised by erythema and edema of the eyelid margin. Telangiectasia may also be present on the anterior eyelid.5 The main stay of treatment involves eyelid hygiene, keeping the lids free from crusts and scales. Warm compresses and light scrubbing of the eyelids are useful. Lid scrubs consisting of saline or diluted mild shampoos can be applied to the affected area. These promote lid hygiene and clear any debris from the lid margin to initiate drainage. Furthermore, ingredients used in shampoos break down bacterial membranes, which helps to further decrease the presence of bacteria at the infection site.6 Topical antibiotics provide symptomatic relief and are effective in clearing bacteria from eyelid margins. Studies have shown no differences between the types of topical antibiotics used.5 In severe cases, oral antibiotics such as doxycycline may be required. Younger children should be prescribed erythromycin instead. Nevertheless, no treatment for blepharitis had been shown to be superior to others, hence patients should always be reminded of the importance of simple measures like eyelid hygiene and warm compresses. Infections of lacrimal system Dacryocystitis Dacryocystitis, an infection of the lacrimal sac, often occurs in patients with underlying nasolacrimal duct obstruction. It develops when bacterial overgrowth occurs in the stagnant fluid of the lacrimal sac. Studies have shown that dacryocystitis might be due to either single isolate or polymicrobial infections.7 Staphylococcus and streptococcus are commonly involved. Patients with dacryocystitis present with a painful swelling over the nasal aspect of the lower eyelid
(Figure 3). They often have a history of chronic tearing due to underlying nasolacrimal duct obstruction. Recurrences are common. Purulent discharge may be expressed by applying pressure over the lacrimal sac. Dacryocystitis may progress into preseptal cellulitis or even orbital cellulitis. Rupture of the abscess, either spontaneous or iatrogenic in nature, may result in fistula formation.8 Treatment includes topical and systemic antibiotics. Intravenous antibiotics are required in severe cases particularly when there is orbital spread, in which case surgical drainage would be the definitive treatment. Patients with underlying nasolacrimal duct obstruction are prone to have recurrences, and may benefit from dacryocystorhinostomy to recanulate the nasolacrimal duct. Infections of conjunctiva Conjunctivitis Conjunctivitis is characterised by dilatation of the conjunctival vessels, resulting in hyperaemia and oedema of the conjunctiva, typically with associated discharge.9 Conjunctivitis can be divided into non-infectious and infectious causes (usually viral or bacterial). Most patients are initially treated by primary care physicians rather than ophthalmologists.10,11 Differentiation between viral and bacterial conjunctivitis may not be easy. In general, purulent or mucopurulent discharge is often due to bacterial
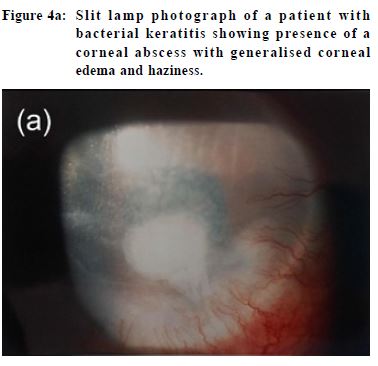
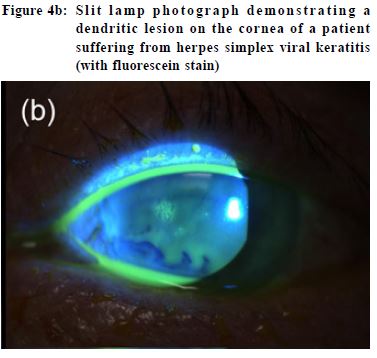
conjunctivitis, whereas a watery discharge is more characteristic of viral conjunctivitis.10 Viral conjunctivitis Viruses cause up to 80% of all cases of acute conjunctivitis.10 Virus spreads through direct contact and is highly contagious especially among children. Viral conjunctivitis is most commonly caused by adenovirus12 and is often bilateral. Patients present with itching, burning and foreign body sensation, redness, and watery discharge in one eye, involving the other within a few days. They often have a history of recent upper respiratory tract infection or contact with other people suffering from conjunctivitis. Examination may reveal palpable pre-auricular lymph nodes may be present. Viral conjunctivitis is usually mild and self-limiting. Most uncomplicated cases resolve in around two weeks. No effective treatment exists, but artificial tears and topical antihistamines may provide symptomatic relief.13 In the past, some clinicians would prescribe antibiotics for patients with viral conjunctivitis in view of the potential for co-infection or superinfection with bacteria. Today, experts hold the view that indiscriminate use of topical antibiotics will promulgate microbial resistance, medication toxicity or allergy.12 Patient education is very important in view of the contagious nature of the disease. Patients should be taught to avoid touching their eyes and sharing their towels with others. Frequent handwashing is necessary. Patients should also be advised of the possible prolonged disease course in terms of weeks to avoid them from expecting fast recovery. Bacterial conjunctivitis The staphylococcal species are the commonest pathogens among adult bacterial conjunctivitis, followed by Streptococcus pneumoniae and Haemophilus influenzae. In children, H influenzae, S pneumoniae, and Moraxella catarrhalis are more prevalent.14 Typical findings include redness, presence of purulent or mucopurulent discharge and chemosis (conjunctival oedema). Hyperacute bacterial conjunctivitis presents with severe copious purulent discharge and decreased vision, often accompanied by eyelid swelling, pain and pre-auricular adenopathy. It is often caused by Neisseria gonorrhoeae. Prognosis is worse and progression is rapid. It is associated with a high risk of corneal involvement and even perforation. Treatment of bacterial conjunctivitis involves use of topical antibiotics. There are no significant differences in achieving clinical cure between any of the broad-spectrum antibiotics eyedrops.10 Factors that influence the choice of antibiotic include local availability, patient allergies, and cost. In Hong Kong, chloramphenicol or levofloxacin eyedrops are often prescribed for simple bacterial conjunctivitis. In cases when gonococcal infection is suspected, treatment requires intramuscular or intravenous ceftriaxone. It is an ocular emergency and should be managed in a timely manner to prevent complications such as corneal perforation. The patient should also be screened for possible sexually-transmitted diseases. Ophthalmia neonatorum Ophthalmia neonatorum, or neonatal conjunctivitis, is defined as conjunctivitis occurring in a newborn during the first month of life. Although it can be viral in nature, sexually transmitted disease agents including Neisseria gonorrhoea and Chlamydia trachomatis are the major causes. Gonococcal conjunctivitis typically presents as sudden, severe, purulent conjunctivitis in the first 3 to 5 days of life.15 If left untreated, progression can be rapid resulting in ulceration, corneal perforation and hence blindness within 24 hours.16 Patients should be hospitalised and prescribed intravenous or intramuscular ceftriaxone. The mother should also be screened and treated for gonorrhoea. Chlamydia conjunctivitis can develop a few days to several weeks after birth, typically at 2 weeks of life. Presentation may vary from scant, mucoid discharge to copious, purulent discharge, conjunctival erythema, ocular edema, chemosis, or pseudomembrane formation.17 There may be associated pneumonitis, otitis media and tracheitis. Treatment involves use of oral erythromycin. Infections of cornea Keratitis This can be caused by bacterial, viral, fungal, parasitic or amoebic infection. In general, patients with keratitis present with a painful red eye, reduced vision and photophobia. The cornea may show a localised ulcer or abscess, and in severe cases the cornea may be diffusely oedematous and hazy (Figure 4a). Conjunctival involvement i.e. keratoconjunctivitis is not uncommon. Corneal ulceration is an ophthalmic emergency and deserves immediate treatment and referral to an ophthalmologist. Nevertheless, the cause of the ulceration must be identified before commencing treatment because while some therapies are beneficial in certain situations, they may worsen the condition in others. For example, while steroid is the main stay of treatment for systemic or autoimmune diseases related keratitis, its inadvertent use may exacerbate infective keratitis particularly viral or fungal keratitis. Viral keratitis Viral keratitis is commonly caused by herpes simplex virus (HSV). The virus produces painful, thin, linear, branching lesions on the corneal epithelium with club-shaped terminal bulbs at the end of each branch, known as a dendritic ulcer (Figure 4b).18 Although HSV epithelial keratitis tends to be self-limiting19, natural healing often takes longer than two weeks.20 Acyclovir eye ointment is used as treatment, and systemic administration has not been shown to be beneficial. Keratitis may occur in around 22-76% of patients with herpes zoster ophthalmicus (HZO).24-27 HZO is the reactivation of varicella zoster virus (VZV) in the ophthalmic division of the trigeminal nerve. Presence of Hutchinson’s sign, i.e. rash involving the tip of the nose due to involvement of the nasociliary branch of the ophthalmic division, signifies a higher risk of ocular involvement. It had been shown that its presence is a reliable prognostic sign of sight-threatening ocular complications in acute HZO.23 Treatment requires use of systemic antiviral drugs. Contact lens keratitis Contact lens wear is a known predisposing factor for microbial keratitis. Pseudomonas aeruginosa is the commonest causative organism, followed by Gram-positive bacteria, fungi and acanthamoeba.28 Patients usually present with eye pain, redness, photophobia, and tearing. They often reveal a history of poor contact lens hygiene, overnight contact lens wear, and swimming or taking a hot water bath while wearing contact lenses. A study had shown that disease load is reduced by 60-70% by avoidance
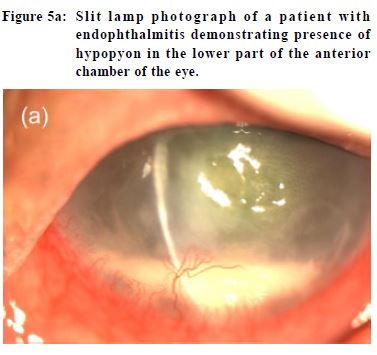
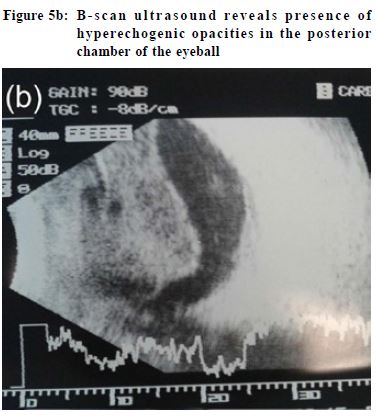
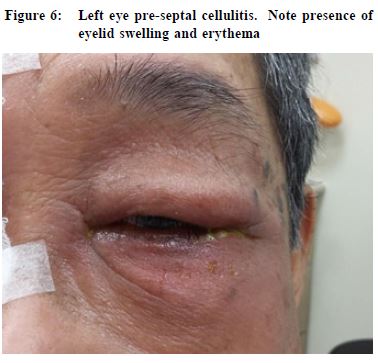
of overnight contact lens use and attention to contact lens hygiene factors.28 Physicians must rule out keratitis in every contact lens wearer consulting for eye redness. Contact lens wearer should be advised to avoid overnight wear and wearing contact lenses while swimming. Good disinfection technique is also essential. Once contact lens keratitis is diagnosed, patients should refrain from contact lens use immediately. A corneal culture is often taken before starting intensive topical antibiotics. Sometimes admission is required for application of intensive fortified antibiotics and close monitoring. Treatment of acanthamoeba is unfortunately often ineffective. Treated contact lens related keratitis may result in formation of corneal scars. In severe non-resolving cases, the cornea may perforate necessitating corneal transplantation. Infection of eyeball Endophthalmitis Endophthalmitis refers to severe intraocular inflammation and the outcome is often devastating resulting in marked visual loss or even blindness. It usually occurs as a result of microbial infection. It can be due to exogenous or endogenous causes. Exogenous endophthalmitis is caused by inoculation of microorganisms from the external environment into the eyeball, most commonly as a complication of penetrating eye trauma and ocular surgery, including but not limited to cataract surgery.29 Endogenous endophthalmitis is caused by hematogenous spread of infectious organisms from distant sites of the body, with Klebsiella urinary tract infection and liver abscess being the commonest sources among the local population.30 Patients with endophthalmitis present with visual blurring, eye pain, eyelid swelling, conjunctival redness, chemosis, and hypopyon (Figure 5a). B-scan ultrasound shows presence of hyperechogenic opacities in the posterior chamber of the eyeball indicating vitreous and posterior involvement (Figure 5b). Prompt diagnosis and hospitalisation is essential because the risk of blindness is very high.30 Cellulitis Orbital (post-septal) cellulitis refers to infection of the tissues posterior to the orbital septum, including the fat and muscle within the bony orbit. Pre-septal cellulitis, on the contrary, refers to involvement of the tissues localised anterior to the orbital septum (including eyelid skin, muscle and superficial periorbital soft tissues). This distinction is important because orbital cellulitis, while less common, may be associated with significant visual and life-threatening sequelae.32 Pre-septal cellulitis may result from trauma, insect bites, underlying eyelid lesions such as chalazion, and iatrogenic causes such as eyelid surgery. Staphylococcus aureus, Streptococcus pyogenes, and Haemophilus influenzae are the common bacteria causing preseptal cellulitis.33
It is characterised by eyelid swelling and erythema (Figure 6). Involvement is superficial and the orbit is not involved. Hence, patients’ vision remains normal and there is no pain on eye movement. Outpatient management with oral antibiotics is the mainstay of treatment. Pre-septal cellulitis may progress posteriorly into the orbit leading to orbital cellulitis. The infection most commonly originates from sinuses, eyelids, dental space, face, retained foreign bodies, or distant sources by hematogenous spread.34 Patients present with eyelid swelling and erythema as in preseptal cellulitis, but since the orbit
is involved, patients also suffer from chemosis, proptosis, blurring of vision, limitation in eye movement, and double vision. If left untreated, orbital cellulitis may result in complications such as formation of periosteal abscess, brain abscess, cavernous sinus thrombosis, meningitis, septicaemia and even death. Hence, orbital cellulitis is an ocular emergency and patients should be referred immediately to an ophthalmologist for hospitalisation. Conclusion For patients with eye infections, many a time when medical care is sought, a general practitioner or a family physician is consulted before an ophthalmologist.2,35 It is therefore important for primary care physicians to be familiar with the common eye infections encountered in daily practice. While many eye infections such as hordeolum and blepharitis are relatively mild and may even resolve spontaneously without treatment, some infections may be severe and may result in permanent visual loss if treated inappropriately. In case of doubt, timely referral to an ophthalmologist is warranted.
Shiu-ting Mak, MBChB(CUHK), MPH(CUHK), FRCSEd(Ophth), FHKAM(Ophthalmology)
Associate Consultant, Department of Ophthalmology, United Christian Hospital Honorary Assistant Professor, Eye Institute, The University of Hong Kong Adjunct Assistant Professor, School of Optometry, The Hong Kong Polytechnic University Honorary Clinical Supervisor, The Hong Kong College of Family Physicians Correspondence to :Dr Shiu - ting Mak , Department of Ophthalmology, United Christian Hospital, 130 Hip Wo Street, Kwun Tong, Kowloon, Hong Kong SAR, China E-mail: dr.makst@gmail.com
References
|
|