September 2010, Volume 32, No. 3 |
Original Articles
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
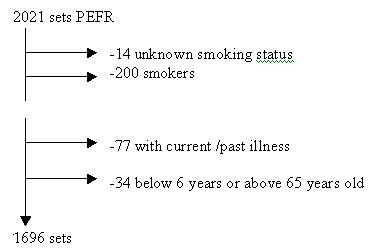
Nomogram of peak expiratory flow rates (PEFR) for Hong Kong ChineseMark SH Chan 陳選豪, Nai-ming Wong 黃乃明, Albert YF Kong 江炎輝, Wilson WS Tam 談維新, Yuk-tsan Wun溫煜讚, Tai-pong Lam 林大邦 HK Pract 2010;32:120-127 Summary Objective: To collect peak expiratory flow rates (PEFRs) of Hong Kong Chinese using the mini-Wright peak flow meters and to construct nomograms in the standardized European (EU) scales. Design: A prospective cross-sectional survey conducted in community based primary care clinics and two schools. 34 family doctors from the 18 districts of Hong Kong collected PEFRs from participants in a one year period. PEFRs were also collected from students of one primary and one secondary schools. The meters used were brand new and their use were standardized. Subjects: Hong Kong Chinese residents aged 6 to 65 years not suffering from conditions that might impair their respiratory function. Main outcome measures: Each participant blew into the flow meter thrice and the best value was taken as the PEFR. His/her height and body weight were taken under standardized condition. Results: Using regression analysis, PEFRs for either sex were best predicted with the model combining age, agesquared, height, and height-squared. The corresponding nomograms were constructed. Conclusion: Sex, age, height and weight were the most important determinants for PEFR from people without apparent impaired respiratory functions. A quadratic equation is best for a predicted PEFR. Keywords: Peak expiratory flow rate, nomogram, Chinese, Hong Kong 摘要 目的:採用Mini-Wright最大流速儀收集中國香港居民的最大呼氣流速值(PEFR),並根據標准化歐洲(EU)量表制成列線圖。 設計:在社區基層醫療診所及2所學校開展一次前瞻性橫斷面調查。來自於香港18個區的34名家庭醫生在一年內收集了參加者的PEFR;還收集了一所小學和一所中學學生的PEFR。所用測量儀器均為新儀器;使用方法經過標准化。 對象:無影響呼吸功能之疾病的6-65 歲的中國香港居民。 主要測量內容:每位參加者對流速儀吹氣三次,取最高值作為PEFR 。在標准條件下測身高及體重。 結果:通過回歸分析,綜合了年齡、年齡平方、身高和身高平方的模型可以最好地預測男性或女性的PEFR。建立相應的列線圖。 結論:性別、年齡、身高和體重是無明顯呼吸功能障礙者PEFR 的最重要決定因素。預測PEFR 最好用二次方程。 主要詞彙:最大呼氣流速,列線圖,中國,香港 Introduction Asthma is a common disease in primary care. In Hong Kong, the prevalence of doctor-diagnosed asthma in children is 11.2%.1 All current international guidelines except the one from National Heart Lung and Blood Institute (USA) still regard peak flow meters (PFM) as an aid to the diagnosis of asthma.2-6 All guidelines find long term PEFR useful in the monitoring of asthma control in adult patients and equally effective as symptom-based monitoring. PEFR is particularly helpful in those patients who have poor perception or confusion of symptoms and in those who have suspected occupational causes. For grading the severity of asthma, a patient’s PEFR or forced expiratory velocity in one second (FEV1) is compared to the predicted value for the patient’s genderand height (or age). Primary care doctors in Hong Kong usually use the mini-Wright peak flow meter (Clement Clarke International) and rarely the spirometer. The predicted values supplied with the meters are not those derived from Hong Kong residents. However, it has been shown that the predicted values for PEFR differ widely among ethnic groups. Ip et al showed that Hong Kong Chinese have lower FEV1 values than the Caucasians, with variations up to 8-12% for different height ranges.7 The wide variations in the predicted values have important implications for primary and emergency care doctors “who must make treatment and disposition decisions for the individual patient”.8 The local data was collected more than 20 years ago when Lam et al published a nomogram of PEFR for Hong Kong Chinese in 1983.9 In 2005, Jones et al found that the PEFR in a sample of university students were at least 10 to 14% lower than the norms developed by Lam et al in 1982.10 Jones et al suggested that changes of the environment in Hong Kong and the physical characteristics of the newer generation individuals affected the local residents’ respiratory function. In 2004, UK and other European countries started using a new ‘standard’ for PEFR (referred to as the new EU scale or EN13826). The PEFR readings taken from the new EU scale are different from those taken from an old Wright-McKerrow scale, and are said to be more accurate as they change uniformly over the whole range of the meter. The new EU scale meters have been introduced into Hong Kong and gradually replaced the old ones. Unfortunately, the conversion table between these two scales is not yet available and one has to interchange the individual readings at the internet web site of Clement Clarke.11 This is most inconvenient for the busy family doctor. Family doctors in Hong Kong very much need an up-to-date nomogram of PEFR for the local residents in the diagnosis and quality-care of our patients with suspected or confirmed asthma. The nomogram in the new EU scale will save much of family doctors' precious time and effort. Our aim is to meet this need in the local family practice by constructing new PEFR nomograms for Hong Kong residents. Method Sampling method This was a prospective cross-sectional survey of persons aged between 6 and 65 years old who had been residing in Hong Kong for at least 12 months. They should be able to give verbal consent (or written consent from parents/guardians for children) and use the mini-Wright peak flow meter after instruction. We excluded those with chronic respiratory disease, concurrent infectious disease of the respiratory tract, or oral / musculoskeletal conditions affecting the respiratory system. We also excluded the PEFR readings if the participant had obviously not blown into the meter with maximum effort. We sent invitation letters to doctors in private practice and recruited 34 family doctors throughout the 18 districts of Hong Kong to participate in the survey. They were to collect as much data as possible over a one-year period (preferably 100 patients each). The doctors were invited to a standardization workshop for briefing on how to use the peak flow meters and how to measure the participants’ body height and weight. Each doctor was given two brand new meters, one with standard range EU scale and one with low range EU scale, together with disposable mouthpieces. Bimonthly reminders through emails and personal contacts were sent throughout the whole period of data collection. To increase the sample size of children and adolescents in our study, we recruited students from one primary school and one secondary school. We made a digital video with the help of the Secondary School Multimedia Group on how to use the peak flow meters and all students viewed the video before blowing into the meter. Instruction for using peak flow meter The technique of blowing in to the PFM was standardized as: (1) Hold PFM so that fingers are clear of the scale and slot (2) Stand upright and hold PFM horizontally (3) Take a deep breath, place PFM in mouth, and close lips around the mouthpiece (4) Blow as hard and as fast as you can (5) Repeat the above procedure twice This technique was demonstrated by the participating doctors before data collection. Participants could practice the technique under supervision using their own disposable mouthpieces and taking a rest of five minutes before the actual data collection. Three readings were recorded from each participant and the best was taken as the PEFR. Instruction on body measurements The body height was measured with each participant standing with the bare feet close together and heels on the ground. The knees, legs and back were kept straight, and the level of the external auditory measured horizontal to that of the lower rim of the orbit. The body weight was taken with the participant in light clothing and without shoes. Statistical analysis Regression analysis was used to construct a prediction equation for PEFR. We used the coefficient of determination, R2, of the regression equations to determine which model was most suitable for the construction of the nomograms. R2 is a measure of how well the dependent variable is explained by the model; in other words, it suggests how well the future outcomes are likely to be predicted by the regression model. Results Sample recruited Of the 34 recruited doctors, over 90% had postgraduate qualifications. At the end of the study, 28 doctors returned a total of 2021 sets of PEFR. We excluded 325 sets: 14 without known smoking status,
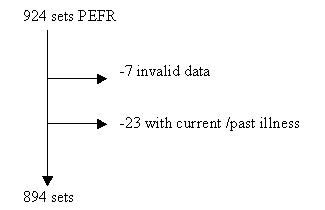
200 current smokers, 77 with illnesses that might affect respiratory function, and 34 either below 6 years or above 65 years old. Only 1696 PEFR values were used for the construction of the nomogram. We recruited students from Forms 1, 3, and 5 at Lok Sin Tong Yu Kan Hing Secondary School on 21st November 2007, and students from Primary 1 to 6 at Lok Sin Tong Leung Kau Kui Primary School on 8th May 2008. The same team of research assistants collected data on both dates. Of the 924 sets of PEFR collected, we excluded seven due to obviously inadequate effort in blowing into the meter, and 23 from students with various illnesses (e.g., history of bronchial asthma) that could affect the PEFR results. Thus, there were 894 sets for analysis.
Overall, there were 2945 (2021+924) participants recruited of whom the data from 2590 (1696 + 894) were used for the nomograms. There were 1188 male participants (45.9%) and 1401 female participants (one missing datum), Table 1.
PEFR and demographic variables PEFR has a linear relationship with body weight, height and BMI, but a curvilinear one with age (Figs 1, 2). Regression analysis Regression analysis shows significant association between PEFR and the following variables: age, height, weight and sex. If we assume a linear relationship, the models with age, height and weight give the highest R2 (0.696 and 0.475 for males and females respectively, Table 2), followed by age + height (0.687 and 0.458 respectively). The association between PEFR and age is a curvilinear one. So, if we assume a quadratic relationship by including the square terms of the variables in the model, the model combining age, age-square (i.e. age x age), height, and height-square (i.e. height x height) gives the highest R2. The corresponding regression equations of PEFR with the highest R2 are in Box 1.
Box 1: Regression equations of PEFR (L/min) for male and female (height in cm and weight in kg). Note that the constant for male PEFR quadratic equation is a positive value.
Normograms Since the models with quadratic equations give the highest R2, we use them to construct the male and female PEFR nomograms (Figs 3, 4). Discussion This survey recruited 2590 local Chinese residents aged 6 to 65 who were non-smokers and free from conditions probably adverse to their respiratory functions. Using mini-Wright peak flow meters of EU scale, we collected their PEFR. The PEFR has significant as sociation with age, sex, body height and weight. Regression analysis shows that, for individual sex, the model of quadratic relationship [with age, age-squared, height, height-squared] gives the best coefficient of determination (R2), followed by linear models of [age, height, weight] and [age, height]. We constructed the PEFR nomograms for both sexes according to the quadratic equations. The nomograms from this survey are useful to the local clinical practice in two ways. More and more practices will use the new EU-scale meters when the old Wright scale meters are phasing off. The nomograms currently available are either not derived from our local population or with local findings more than twenty years ago; they might not be valid now. Our nomograms will serve as an updated reference for the predicted PEFR values based on the new scale. The previously only available PEFR nomograms for Hong Kong residents were from Lam et al.9 In their series of 3490 residents, 747 were current smokers, 163 had history of wheezes, 361 had history of dyspnoea and 154 had chest conditions like old tuberculosis, comprising 40% of the total sample population. They found that the PEFR differed significantly between smokers and non-smokers, and between those with and those without sputum production. In our study we excluded these recruited participants. We believe that our nomograms are more likely to be closer to the true predicted values from people without conditions that could adversely affect PEFR. We could identify only two reports of PEFR of the general population in Southern China9,12 in the literature. The one by Lam et al in Hong Kong found PEFR best regressed against body height, age and age3. The one by Chung et al in Guangzhou found PEFR best regressed against body height, age, age2, and age3. Thus, like ours, both found a quadratic regression equation to be most fit. But in both of these reports, the R2 was around 0.40, much below that of this study. Similar to both reports, this study also found that females reached their maximum PEFR values earlier than males. The recruited participants of this study were a convenient sample. Such sampling method is perhaps the best we could do for a survey of such nature and within our resources. We succeeded in soliciting the help from doctors over the 18 districts of Hong Kong so that the recruited population came from widely distributed residential areas. We recruited more children and adolescents by involving two schools because we wished to increase the validity of the predicted values in this age group. Bronchial asthma is more common in this age group and the predicted PEFR values are more helpful in the management of children. Incidentally, by involving these schools, we delivered health education about asthma and the use of peak flow meters to the students, a benefit that was not anticipated before the study. Conclusion A prospective cross-sectional survey was conducted in the community based primary care setting to collect peak expiratory flow rate of the Hong Kong Chinese. Sex, age, height and weight were the most important determinants for PEFR from people without apparent impaired respiratory functions. A quadratic equation is best for a predicted PEFR. New nomograms were constructed based on the result and should replace the nomograms based on data collected in the 1980s. Acknowledgement We would like to thank the following persons/institutions for their help in our research:
Key messages
Mark SH Chan, MPainMed, DFM, FHKCFP, FRACGP Nai-ming Wong, MBBS, DOM, FHKCFP, FRACGP Albert YF Kong, FRCP, FHKCFP, FRACGP, FHKAM(Paed) Wilson WS Tam, PhD Yuk-tsan Wun, MD(HKU), FHKCFP, FRACGP, FHKAM(Fam Med) Tai-pong Lam, PhD(Sydney), MD(HKU), FRCP, FHKAM(Fam Med) Correspondence to: Dr Mark SH Chan Shop 27, G/F, Flora Plaza, Fanling, NT, Hong Kong SAR. E-mail: drmchan@netvigator.com References
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||